-
Title
-
Deep Brain Stimulation for Psychiatric Disorders
-
Author
-
Widge, Alik S.
-
Arulpragasam, Amanda R.
-
Deckersbach, Thilo
-
Dougherty, Darin D.
-
Research Area
-
Psychopathology
-
Topic
-
Mental Illness Diagnosis and Treatment
-
Abstract
-
In this monograph, we briefly review the rationale for deep brain stimulation (DBS) for psychiatric illness, beginning with current noninvasive treatment options and progressing to the evolution and success of DBS as a therapy. This discussion will focus on obsessive‐compulsive disorder (OCD) and major depressive disorder (MDD) particularly, as these are the only two diagnoses that have been subjected to adequately controlled DBS trials to date. The majority of the essay then describes the significant limitations that DBS is currently facing and emerging approaches to address them. This will lead into a discussion of new technologies such as patient‐specific modeling of electric fields and closed‐loop DBS systems and how we can best utilize these to increase our understanding of DBS and the overall efficacy of this novel therapy.
-
Related Essays
-
Positive Emotion Disturbance (Psychology), June Gruber and John Purcell
-
What Is Neuroticism, and Can We Treat It? (Psychology), Amantia Ametaj et al.
-
Peers and Adolescent Risk Taking (Psychology), Jason Chein
-
Delusions (Psychology), Max Coltheart
-
Misinformation and How to Correct It (Psychology), John Cook et al.
-
Problems Attract Problems: A Network Perspective on Mental Disorders (Psychology), Angálique Cramer and Denny Borsboom
-
Controlling the Influence of Stereotypes on One's Thoughts (Psychology), Patrick S. Forscher and Patricia G. Devine
-
Depression (Psychology), Ian H. Gotlib and Daniella J. Furman
-
Mental Imagery in Psychological Disorders (Psychology), Emily A. Holmes et al.
-
Normal Negative Emotions and Mental Disorders (Sociology), Allan V. Horwitz
-
Dissociation and Dissociative Identity Disorder (DID) (Psychology), Rafaële J. C. Huntjens and Martin J. Dorahy
-
Computer Technology and Children's Mental Health (Psychology), Philip C. Kendall et al.
-
Cultural Neuroscience: Connecting Culture, Brain, and Genes (Psychology), Shinobu Kitayama and Sarah Huff
-
Mechanisms of Fear Reducation (Psychology), Cynthia L. Lancaster and Marie-H. Monfils
-
Disorders of Consciousness (Psychology), Martin M. Monti
-
Cognitive Bias Modification in Mental (Psychology), Meg M. Reuland et al.
-
Clarifying the Nature and Structure of Personality Disorder (Psychology), Takakuni Suzuki and Douglas B. Samuel
-
A Gene-Environment Approach to Understanding Youth Antisocial Behavior (Psychology), Rebecca Waller et al.
-
Rumination (Psychology), Edward R. Watkins
-
Identifier
-
etrds0103
-
extracted text
-
Deep Brain Stimulation for
Psychiatric Disorders
ALIK S. WIDGE, AMANDA R. ARULPRAGASAM,
THILO DECKERSBACH, and DARIN D. DOUGHERTY
Abstract
In this monograph, we briefly review the rationale for deep brain stimulation (DBS)
for psychiatric illness, beginning with current noninvasive treatment options and
progressing to the evolution and success of DBS as a therapy. This discussion will
focus on obsessive-compulsive disorder (OCD) and major depressive disorder
(MDD) particularly, as these are the only two diagnoses that have been subjected to
adequately controlled DBS trials to date. The majority of the essay then describes
the significant limitations that DBS is currently facing and emerging approaches
to address them. This will lead into a discussion of new technologies such as
patient-specific modeling of electric fields and closed-loop DBS systems and how
we can best utilize these to increase our understanding of DBS and the overall
efficacy of this novel therapy.
INTRODUCTION: THE RATIONALE FOR DBS IN PSYCHIATRY
The most common treatments for psychiatric disorders are medications and
psychotherapy. However, several large scale studies have shown that even
best-evidence treatment fails to help a substantial fraction of patients (Manschreck & Boshes, 2007; Warden, Rush, Trivedi, Fava, & Wisniewski, 2007).
Obsessive-compulsive disorder (OCD) is a chronic psychiatric disorder
that affects approximately 3% of the world’s population. Presently, first-line
treatment options include cognitive-behavioral therapy and medications
such as serotonergic reuptake inhibitors (SSRIs) (Koran, Hanna, Hollander,
Nestadt, & Simpson, 2007). Approximately one third of patients may not
experience substantial benefit despite receiving both medication and behavioral therapy (Kronig et al., 1999). Major depressive disorder (MDD) is one of
the leading causes of disability in the world and affects approximately 14.8
million American adults with a lifetime prevalence rate of 19.2% (Bromet
et al., 2011). It is estimated that 50–60% of these patients fail to fully respond
to an antidepressant in which adequate dosing and duration have occurred
Emerging Trends in the Social and Behavioral Sciences. Edited by Robert Scott and Stephen Kosslyn.
© 2015 John Wiley & Sons, Inc. ISBN 978-1-118-90077-2.
1
�2
EMERGING TRENDS IN THE SOCIAL AND BEHAVIORAL SCIENCES
(Fava, 2003). For depression, other options such as electro-convulsive
therapy (ECT) or transcranial magnetic stimulation (TMS) also exist. For
OCD, once medications and intensive therapy have failed, patients have few
further treatment options.
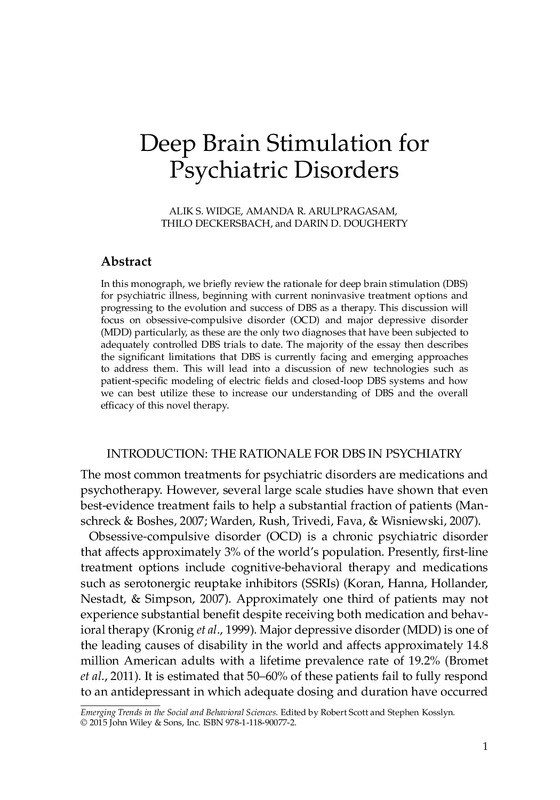
During the last 10–15 years, we have witnessed a major paradigm shift
in the conceptualization of psychiatric disorders (Mayberg, 2009). Basic
research has significantly advanced our understanding of the anatomy
and physiology of brain networks and their mechanisms for processing
cognition, behavior, and emotion. An example of such a circuit can be shown
in Figures 1 and 2. The advancement of our knowledge in neural circuitry
has had a major impact by transforming our understanding of psychiatric
pathophysiology, and has also set the stage for new treatment modalities
that directly modulate disease-relevant circuits (Arulpragasam et al., 2013).
One such treatment that has been shown to modulate maladaptive circuitry
is DBS. DBS is a nonlesion-based, reversible neuromodulation therapy. DBS
Exteroception
-Attention
-Appraisal
-Action
Mood regulation
-Attention
-Appraisal
-Action
mFC
PFC
PMC
ParC
MCC
dpHC
PCC
VS-CDT
dmTH
AMYG
MB-VTA
pACC
mOFC
SCC
AntIns
Mood monitoring
-Novelty
-Salience
-Habit
va-HC
HTH
BS
Interoception
-Drive states
-Autonomic function
-Circadian rhythms
Figure 1 The functional neurocircuitry of obsessive-compulsive disorder (OCD)
as described by Corse et al. 2013. Hypoactivity of the cortico-striatal-thalamiccortical (CSTC) loop (between the OFC and striatum) or hyperactivity of the
corticothalamic (CT) loop (between the OFC/PFC and the thalamus) may result in
OCD symptoms. ACC = anterior cingulate cortex; OFC = orbitofrontal cortex;
PFC = prefrontal cortex.
�Deep Brain Stimulation for Psychiatric Disorders
3
Negative
feedback
loop (−)
Striatum
Thalamus
CSTC
CT loop (+)
OFC
PFC
Frontal
cortex
ACC
Limbic
system
Figure 2 Circuit model of MDD. Adapted from Mayberg, 2009. Regions with
known anatomical interconnections that show consistent changes across
converging imaging experiments form the basis of this model. Regions are
grouped into four main compartments, reflecting general behavioral dimensions of
MDD and regional targets of various antidepressant treatments. Regions within a
compartment all have strong anatomical connections to one another. Black arrows
identify cross-compartment anatomical connections. Solid colored arrows identify
putative connections between compartments mediating a specific treatment.
AntIns = anterior insula; AMYG = amygdala; BS = brainstem; dmTH = dorsomedial
thalamus; dpHC = dorsal-posterior hippocampus; HTH = hypothalamus;
MB-VTA = midbrain-ventral tegmental area; MCC = medial cingulate cortex;
mFC = medial frontal cortex; mOFC = medial orbital frontal cortex; pACC = the
perigenual area of the anterior cingulate cortex; ParC = parietal cortex; PCC =
posterior cingulate cortex; PFC = prefrontal cortex; PMC = premotor cortex;
va-HC = ventral-anterior hippocampus; SCC = subcallosal cingulate; VS-CDT =
ventral striatum-caudate.
involves surgically implanting electrodes at specific target locations within
the brain and delivering electrical pulses of adjustable frequency and
intensity through those electrodes (Corse et al., 2013). In the early 1960s, it
was shown that electrical stimulation of the ventrolateral thalamus could
alleviate tremor (Hassler, Riechert, Mundinger, Umbach, & Ganglberger,
1960) and in the early 1990s, DBS was further developed for the treatment
of essential tremor and Parkinson’s disease (PD) (Benabid et al., 1991). Since
then, the safety and efficacy of DBS for movement disorders such as PD,
essential tremor and extrapyramidal dyskinesia has been repeatedly demonstrated in rigorous clinical trials (Deuschl et al., 2006; Mueller et al., 2008).
The FDA approved the use of DBS for PD in 2002, and since then, over 70,000
patients have undergone DBS for this specific indication (Bronstein et al.,
2011).
�4
EMERGING TRENDS IN THE SOCIAL AND BEHAVIORAL SCIENCES
The success of DBS in modulating pathological circuitry in movement disorders suggests that it may be a viable option for treating disorders that result
from maladaptive changes in brain circuits leading to pathological processing of affective and behavioral information, in patients who do not respond to
medication, psychotherapy, or other less invasive treatment modalities. This
definition of “maladaptive changes in brain circuits” encompasses most, if
not all, psychiatric disorders. As such, exploration and investigation of the
potential benefits of DBS in refractory psychiatric illness is justified.
FOUNDATIONAL AND CUTTING-EDGE WORK: STATE OF THE
ART OF DBS IN PSYCHIATRY
DBS was first investigated by Nuttin and colleagues in 1999 (Nuttin, Cosyns,
Demeulemeester, Gybels, & Meyerson, 1999) in patients with refractory
OCD, in what was also the first ever recorded case series of DBS performed
specifically for a psychiatric indication. This early report prompted ongoing
investigations, which continued to demonstrate similar, successful results
(Abelson et al., 2005; Gabriels, Cosyns, Nuttin, Demeulemeester, & Gybels,
2003). The internal capsule site most commonly studied for OCD is derived
from the location for ablative procedures for treatment-resistant OCD and
anterior capsulotomy (Corse et al., 2013) DBS at this site was expected
to modulate of circuitry specifically implicated in the pathophysiology
of OCD.
Over time, the target moved to a location slightly more posterior than a
traditional capsulotomy. This new location is thought to be the junction of
the anterior commissure, internal capsule, and striatum (Greenberg et al.,
2010), and thus is called the “ventral capsule/ventral striatum” (VC/VS).
At this target, the mean improvement in Yale-Brown Obsessive-Compulsive
Scale (YBOCS) score was 38%, from 34 to 21 (Greenberg et al., 2010) Depression also improved, with a mean drop of 43% in Hamilton Depression Rating Scale (HDRS) and 50% of patients meeting criteria for depressive remission (HDRS < 7) at their last follow-up visit (Kaur et al., 2013) These positive
results led to the US Food and Drug Administration approving (on a limited
basis) DBS for treatment-resistant OCD at the VC/VS target in 2009 (Corse
et al., 2013). This was the first and remains the only approval for use of DBS
for a refractory psychiatric illness in nonresearch practice.
Intriguingly, DBS at VC/VS seemed to also alleviate comorbid depression.
Thus, Malone et al. (2009) conducted the first VC/VS DBS open-label, multicenter trial for treatment resistant depression (TRD) at three collaborating
clinical sites: the Cleveland Clinic, Butler Hospital/Brown Medical School,
and the Massachusetts General Hospital. This pilot study demonstrated a
40% MDD remission rate. An expanded cohort reported in 2010 showed
�Deep Brain Stimulation for Psychiatric Disorders
5
similar results, with a 71% response rate at the last follow-up (Malone,
2010). Surprisingly, a multi-center randomized trial conducted following
these open-label reports did not reach significance and was stopped because
of interim analyses [D. Dougherty, unpublished results]. In parallel, the
Mayberg-Lozano group at the University of Toronto and Emory University
conducted a very similar trial at a different target, the subgenual cingulate
gyrus (Cg25) (Mayberg et al., 2005). That target was rationally selected based
on over a decade of neuro-imaging studies, and had also shown positive
open-label results (Mayberg, 2009). Despite this, the Cg25 trial also failed to
achieve its primary endpoint.
THE CRITICAL NEED: GREATER UNDERSTANDING FOR TRULY
EFFECTIVE DBS
These previous studies demonstrated the promise of DBS in the field of neuropsychiatry, but also highlighted its current shortcomings. It is clear that the
research community has not yet identified the anatomic targets or electrical
parameters that can deliver on that promise. There is much more we need to
know and investigate to optimize DBS.
First, a better understanding of how DBS works and how this stimulation
actually affects individual neurons and larger brain circuitry would enable
more rational therapeutic design. As described above, most DBS targeting is
based on anatomy—on regions that are hyper-active during brain imaging or
where neurosurgeons have successfully treated disease by lesioning tissue.
The clinical trials have shown us that it is not enough to have the electrode
in the right part of the brain. Instead, we need to understand what exactly
the electrical stimulation is doing to the neurons in that tissue, and how the
signal might be propagating through the complex circuitry of the brain.
Secondly, state of the art DBS devices are open loop systems. Present DBS
systems deliver energy continuously at a pre-programmed frequency and
amplitude, with parameter adjustments only occurring during relatively
infrequent clinical programming visits (roughly every 3 months) (Widge,
Dougherty, & Moritz, 2014). DBS needs to progress to becoming “closed
loop”—to being able to monitor its efficacy in real-time and to automatically
adjust stimulation in response to that monitoring. While these systems have
demonstrated therapeutic benefit, they incorrectly assume that psychiatric
symptoms are static. Clinically symptoms of many disorders vary day to
day or moment to moment. Systems that can monitor and respond to these
changing symptoms may have greater tolerability or better response rates.
Lastly, psychiatric diagnoses may not map well to brain entities that can
be targeted through DBS. The categorical nature of psychiatric diagnosis
means that two patients with the same disorder may have very little overlap
�6
EMERGING TRENDS IN THE SOCIAL AND BEHAVIORAL SCIENCES
in symptoms. Further, most patients with severe psychiatric disorders have
co-occurring diagnoses. Symptoms overlap across diagnostic boundaries.
Therefore, a trans-diagnostic approach that focuses on underlying functional
dimensions may improve the mapping between symptoms and neural activity. The remaining portion of this essay will expand on these three points
and provide insight and ideas as to how we believe the field can move
forward.
EMERGING TREND: DEEPER UNDERSTANDING OF THE NEURAL
MECHANISMS OF DBS
To improve the efficacy of DBS, we must better understand its underlying
mechanism of action. Previously, it was thought that DBS merely simulated
the effect of lesioning tissue (Bronstein et al., 2011). However, we now believe
the mechanism to be much more complicated.
While the exact mechanism of action remains unknown, there are several
current theories. McIntyre, Grill, Sherman, & Thakor (2004) noted that several
experimental studies have produced contradictory results, showing inhibition of activity in the stimulated target, but increased inputs to projection
nuclei. To explain these seemingly opposite findings, they studied stimulation using a computational model that incorporated representations of a
clinical DBS electrode and a thalamocortical relay neuron.
They found that the response of the neuron to DBS was primarily dependent on the position and orientation of the axon with respect to the electrode
and the parameters of stimulation (McIntyre et al., 2004). Intracellular stimulation applied within the cell body generated action potentials that were
transmitted down the axon with the same stimulus frequency. However,
extracellular DBS (the actual modality used clinically) resulted in independent firing of the cell body and axon at high stimulation frequencies. This
suggests that during high frequency stimulation, cell body activity may be
decoupled from axonal activity, and a single neuron may simultaneously be
inhibited at its soma (where it receives input from other cells) and excited in
its axon (its output to downstream cells) (McIntyre et al., 2004). This creates
an “information blockade”—there is no meaningful relationship between
the firing of cells upstream of the stimulated neuron and the output that the
neuron sends to its targets. It is no longer able to perform a computational
function. Depending on where the stimulated neuron falls in a brain circuit,
this could act as a lesion of the tissue, or it could act as though the stimulated
nucleus were hyperactive. Detailed computer modeling of DBS is continuing
to emerge as a powerful technique to enhance our understanding of the
effects of DBS and to create a virtual test platform for novel stimulation
strategies (McIntyre & Foutz, 2013). The next step will be expanding this
�Deep Brain Stimulation for Psychiatric Disorders
7
modeling to a wide range of tissues and electrode configurations, a task
which will be mathematically and computationally difficult.
Alongside computational modeling, there is growing interest in recording while using DBS in patients to better understand the underlying neural
mechanism of DBS. Figee et al. (2013) used functional magnetic resonance
imaging (fMRI) and electroencephalography (EEG) to investigate nucleus
accumbens (NAc) DBS in 16 OCD patients. By alternating between a DBS
ON and DBS OFF state, they were able to measure differences in NAc activity
as a result of stimulation. During DBS OFF, the NAc activity in patients was
lower than in controls, whereas during DBS ON, patients had similar NAc
activity as healthy controls (Widge et al., 2014). This suggests that DBS has the
capacity to normalize NAc activity—the exact opposite of the classical “lesion” hypothesis. They also found that DBS targeted at the NAc within OCD
patients reduced excessive connectivity between the NAc and prefrontal cortex (PFC) and also attenuated the increase in low-frequency PFC activity
elicited by symptom provocation (Figee et al., 2013). Thus, there is support
for a theory that DBS may act in psychiatric illness not by modulating a single brain area, but instead by altering connectivity patterns between multiple
areas.
Using a similar method of alternating between DBS ON and DBS OFF
states, Cavanagh et al. (2011) measured changes in subthalamic nucleus
(STN) activity through EEG in patients with STN DBS for PD (Cavanagh
et al., 2011). They used a reinforcement learning and choice conflict task in
which participants were asked to select between novel stimulus combinations involving low (win–lose) or high (win–win and lose–lose) decision
conflict (Cavanagh et al., 2011). They found that during the DBS ON condition, patients responded faster when making suboptimal (poorer) choice
than when making optimal choices. There was no difference in response
time during the DBS OFF condition (Cavanagh et al., 2011). In other words,
DBS of this site caused a subtle psychiatric symptom—a tendency toward
premature responding that drove them to make poor, impulsive choices.
EEG recordings in the medial PFC (mPFC) predicted slower response times
during high-conflict trials in healthy control participants and patients in
the DBS OFF condition, but not in the DBS ON state (Cavanagh et al.,
2011). Here again, it appears that multiple structures (at least mPFC and
STN) are communicating in a network to produce a cognitive phenomenon
(decision-making), and DBS can alter that communication to produce
behavior change.
As the available base of patients with DBS at different brain sites increases,
studies such as these will become increasingly feasible. Furthermore,
advances in imaging and recording technology, along with signal processing, will make it easier for neuroscientists to interpret the findings of these
�8
EMERGING TRENDS IN THE SOCIAL AND BEHAVIORAL SCIENCES
studies. It can also be expected that there will be more and better behavioral
tasks developed, which will help us understand how DBS of each brain
region subtly alters patients’ behavior. The clinical use of DBS according to
anatomic targeting rules will help us produce the neuroscientific data that
will lead to much more rational targeting and programming.
A closely related trend is patient-specific modeling of the spread of the
electric field and its effects on cells and circuits. Riva-Posse et al. (2014) used
diffusion tensor imaging (DTI, a method of mapping connections in the
brain) to model white matter connections and identify the pathways that
govern DBS response for depression. In this study, preoperative MRI data,
including DTI, were acquired in 16 TRD patients. The patients then received
DBS implants at the subcallosal cingulate (Cg25) target. Postoperatively,
computerized tomography was used to locate DBS contacts. The activation
volume around the contacts used for stimulation was then modeled for each
patient and patient-specific tract maps were calculated (Riva-Posse et al.,
2014). The patients were then clinically assessed for therapeutic response at
6 months and 2 years post implant. DBS responders at 6 months (n = 6) and
2 years (n = 12) shared bilateral pathways from their individual activation
volumes to the medial frontal cortex, rostral and dorsal cingulate cortex, and
subcortical nuclei. Nonresponders, on the other hand, did not show these
connections consistently (Riva-Posse et al., 2014). This is a preliminary, but
exciting result—it suggests that it may be possible to define, for each individual patient, the exact anatomic coordinates that would place their DBS at a
“hub” connected to a wide variety of brain areas. If the network-modulation
hypothesis is correct, DBS at a highly-connected hub should be much more
effective. Future years will hopefully show us prospective tests of this
method.
EMERGING TREND: CLOSING THE LOOP
Psychiatric symptoms are not static. Symptoms flare and subside, on a
timescale of minutes to hours. Existing DBS strategies have been unable
to effectively treat such fluctuations, because they occur on significantly
shorter timescales than the relatively infrequent clinical programming
visits. It has been proposed that the stimulator could become “closed
loop”—it could actively monitor the patient’s current emotional state, then
adjust stimulation to compensate. Ideally, stimulation could go from the
present paradigm continuous operation (always on, fixed parameters) to
an intermittent, responsive mode (on only when the patient needs it, with
dynamically adjusting paramters) (Widge et al., 2014). In many ways, this
is the same problem as brain-computer interfaces (BCIs), a technology
currently used to treat paralysis by “decoding” movement commands
�Deep Brain Stimulation for Psychiatric Disorders
9
from the motor cortex. In a psychiatric DBS, the BCI would continuously
monitor emotional state and adjust stimulation parameters to maintain the
patient in an optimal range (Widge et al., 2014). The emotional state signals
are already established to occur within the brain, particularly within the
PFC, which specifically serves emotional regulation functions (Hamilton
et al., 2012). A responsive system would assume some of that regulatory
function to compensate for circuits that have become either dysfunctional
or hypofunctional. Moreover, it would deliver electrical stimulation that is
appropriate to the patient’s immediate need. This would in turn reduce the
side effects associated with over-stimulation, alleviate residual symptoms
related to under-stimulation, and optimize power consumption, leading to
slower battery depletion (Widge et al., 2014). Major funding agencies in the
United States have committed to developing these closed-loop systems,1 and
DBS manufacturers have already released hardware that could implement
them (Afshar et al., 2013).
The development of closed-loop emotional DBS is a promising new
approach but it has been hindered by a lack of feasible electrical biomarkers.
That is, it is unknown what the electrical signature of psychiatric illness
or remission looks like within the brain. Until we know what the DBS
should sense, it is difficult to build a closed-loop controller that decodes
critical psychiatric information from neural firing. fMRI can provide insights
into activity across the whole brain (Sitaram et al., 2011), however, most
fMRI sequences are not fully compatible with DBS implanted devices and
thus, unfortunately, cannot be utilized. Second, decoding modalities that
support continuous recording may not function properly in the presence of
psychiatric disorders (Widge et al., 2014). EEG has been a very successful
method for noninvasive emotion decoding in human volunteers (Kim, Kim,
Oh, & Kim, 2013). However, all successful EEG emotion decoding has only
been shown in healthy control participants. Patients with mental illness,
by definition, do not have normal neural circuits or activation. Therefore,
measures that accurately classify healthy controls may not transfer over to
this population. Furthermore, there is a consensus that clinical diagnoses
oftentimes contain multiple neurologic entities and that the same clinical
phenotype might arise from diametrically opposite changes in the brain
(Cuthbert & Insel, 2013). This could present a potential challenge for clinical
translation of existing emotional decoders (Widge et al., 2014). Third, even
if BCIs are able to function in the presence of clinical symptoms, they
may not be able to adequately distinguish pathologic states from normal
states (Widge et al., 2014). Psychiatric disorders are marked by extremes
of emotions that are normally occurring in everyday life. The difference
1. http://www.technologyreview.com/news/527561/military-funds-brain-computer-interfaces-tocontrol-feelings/. [cited 2014 Jun 14].
�10
EMERGING TRENDS IN THE SOCIAL AND BEHAVIORAL SCIENCES
is not severity or type, but rather its context and appropriateness in a
given situation. In post-traumatic stress disorder (PTSD) for example,
patients may overgeneralize from a fearful event and later experience high
vigilance and arousal in contexts that are objectively safe. The question is
differentiation—can we tell whether a patient is having a PTSD flashback
(where the BCI-DBS system should intervene to reduce his/her fear) or
watching a thrilling movie (where the BCI-DBS should allow the patient
to enjoy this normal and healthy human experience)? A system that fails
to distinguish could actually be more harmful than the symptoms it seeks to
treat.
The search for those biomarkers will be a critical trend in DBS research
in the coming decade. However, equally important is the question of
whether we might be able to create a closed-loop DBS while foregoing
biomarkers entirely. Recent demonstrations have suggested a completely
new approach—direct volitional control of the neurostimulator. In such a
device, a patient would sense that current stimulation parameters are not
well matched to his/her clinical needs, then directly communicate this to
the stimulation by deliberately modulating specific aspects of brain activity
(Widge et al., 2014). This is even more directly a use of the BCI technologies
described above—those technologies were developed for exactly this kind
of “intention decoding”. In this scenario, we would not need to worry
about the BCI’s ability to classify an emotion as pathologic vs. healthy—the
patient would “tell” the stimulator directly whether the current emotional
experience was desirable or undesirable. This could occur in real-time,
changing stimulation moment-to-moment to track experienced symptoms,
rather than waiting weeks between programming visits. Heterogeneity of
biomarkers would also be a moot point – the only important variable would
be the patient’s own intention to receive mood-altering stimulation (Widge
et al., 2014). A proof-of-concept demonstration of this approach has recently
occurred in an animal model. Rats have used such a system to directly
trigger stimulation to the medial forebrain bundle (MFB), a structure within
the reward pathway where electrical stimulation is known to be reinforcing
(Widge & Moritz, 2014). This volitional pathway to closed-loop DBS has
much work to be done before it becomes a clinical reality, but offers the
exciting possibility that patients could literally regain their capacity for
self-control.
EMERGING TREND: RATIONAL DESIGN AND TRIALS OF
PSYCHIATRIC NEUROTHERAPEUTICS
In discussing the potential for closed-loop systems, we have described the
present lack of identified, treatable neural biomarkers of DSM disorders. One
�Deep Brain Stimulation for Psychiatric Disorders
11
reason for this is that symptom-based psychiatric diagnoses may not be neurological entities (Cuthbert & Insel, 2013; Insel & Wang, 2010). That is, if a
single disorder/diagnosis can be achieved by a wide variety of symptom
clusters, it is reasonable to believe that those clusters might be produced
by a variety of underlying problems in brain structures and circuits. If this
is true, the failure to find a neurological basis of psychiatric illness is not
surprising—a search for specific brain dysfunction cannot lead to significant
findings if only a small subset of studied patients actually have that dysfunction. To produce a clearer picture of the mapping between symptoms and
neural activity, we likely need to move away from focusing on categorical
diagnoses which lead to extraneous overlap and instead focus on modeling,
targeting and treating the functional problems that underpin those diagnoses
(Cuthbert & Insel, 2013; Insel, 2014).
There are known correlates and behavioral tests for working memory (Gazzaley & Nobre, 2012), impulsivity (Bari & Robbins, 2013), emotion regulation
(Price & Drevets, 2012), and many other behaviors that cut across mental illnesses. Instead of treating heterogeneous disorders, one could develop tests
for those functional domains, and then target stimulation to domain-specific
symptoms and circuits. Doing so would address what is actually pathological
for each individual patient. Furthermore, moving to a domain-oriented diagnosis and treatment system would better leverage extensive animal work
in brain stimulation. Psychiatric treatment screening in animals is limited,
because there is no evidence that animal behavioral tests produce analogues
of human emotion. There is, however, proof for observable behavior changes
on standardized tests. A transdiagnostic approach would focus on what can
be precisely measured in both animals and humans, and could thus allow us
to treat real, quantifiable phenomena.
One such example for the application of this new approach is extinction
learning. There is a rapidly evolving literature on fear extinction and
the fear-safety learning network, which includes the ventromedial PFC,
amygdala and hippocampus (Marin, Camprodon, Dougherty, & Milad,
2014; Milad & Rauch, 2007; Milad et al., 2007). There is considerable overlap
between this fear extinction network and several brain regions associated
with symptom severity in psychiatric illnesses such as OCD, MDD and most
notably, PTSD (Marin et al., 2014; Milad et al., 2008). This suggests that if we
could work out a DBS that specifically targeted the fear network (leveraging
the emerging evidence on network effects of DBS), that single intervention
could be applicable to numerous mental disorders (Marin et al., 2014).
This transdiagnostic approach would face numerous hurdles. Most of
the existing scientific literature is disease/disorder oriented, making it
difficult to re-tool studies to address domains. Further, there would be
substantial regulatory hurdles—at least in the United States, devices are
�12
EMERGING TRENDS IN THE SOCIAL AND BEHAVIORAL SCIENCES
usually approved to treat specific diagnoses. Funding agencies have begun
to propose the transdiagnostic approach, (Insel, 2014) but it will be some
time before this idea is well adopted, let alone suitable for use in clinical
practice. Nevertheless, this represents the progression of psychiatry (and
interventional psychiatry in particular) into a genuinely rational field, and
is a trend to be encouraged.
CONCLUSIONS
DBS for psychiatric illness has had great promise, but has stumbled in
converting that promise to clinical reality. Much of that relates to a lack
of understanding—of the mechanisms of action, biomarkers of efficacious
treatment, and the appropriate selection of patients/impairments to be
treated with implantable devices. Numerous investigators are actively
researching solutions to these problems, and the next decade promises great
advances.
REFERENCES
Abelson, J. L., Curtis, G. C., Saqher, O., Albucher, R. C., Harrigan, M., Taylor, S. F., … ,
Giordani, B. (2005). Deep brain stimulation for refractory obsessive-compulsive
disorder. Biological Psychiatry, 57(5), 510–516.
Afshar, P., Khambhati, A., Stanslaski, S., Carlson, D., Jensen, R., Linde, D., … ,
Denison, T. (2013). A translational platform for prototyping closed-loop neuromodulation systems. Front Neural Circuits, 6: 117.
Arulpragasam, A. R., Chou, T., Kaur, N., Corse, A. K., Deckersbach, T., &
Camprodon, J. A. (2013). Future directions of deep brain stimulation: current disorders, new technologies. Psychiatric Annals, 43(8), 366–373.
Bari, A., & Robbins, T. W. (2013). Inhibition and impulsivity: Behavioral and neural
basis of response control. Progress in Neurobiology, 108, 44–79.
Benabid, A. L., Pollak, P., Gervason, C., Hoffmann, D., Gao, D. M., Hommel, M. … ,
de Rougeont, J. (1991). Long-term suppression of tremor by chronic stimulation of
the ventral intermediate thalamic nucleus. Lancet, 337(8738), 403–406.
Bromet, E., Andrade, L. H., Hwang, I., Sampson, N. A., Alonso, J., de Girolamo, G.,
… , Kessler, R. C. (2011). Cross-national epidemiology of DSM-IV major depressive
episode. BMC Medicine 9: 90.
Bronstein, J. M., Taqliati, M., Alterman, R. L., Lozano, A. M., Volkmann, J., Stefani,
A., … , DeLong, M. R. (2011). Deep brain stimulation for parkinson disease: An
expert consensus and review of key issues. Archives of Neurology, 68(2), 165.
Cavanagh, J. F., Wiecki, T. V., Cohen, M. X., Figueroa, C. M., Samantha, J., Sherman,
S. J., & Frank, M. J. (2011). Subthalamic nucleus stimulation reverses mediofrontal
influence over decision threshold. Nature Neuroscience, 14(11), 1462–1467.
Corse, A. K., Chou, T., Arulpragasam, A. R., Kaur, N., Deckersbach, T., & Cusin,
C. (2013). Deep brain stimulation for obsessive-compulsive disorder. Psychiatric
Annals, 43(8), 351–357.
�Deep Brain Stimulation for Psychiatric Disorders
13
Cuthbert, B. N., & Insel, T. R. (2013). Toward the future of psychiatric diagnosis: The
seven pillars of RDoC. BMC Medicine, 11, 126.
Deuschl, G., Schade-Brittinger, C., Krack, P., Volkmann, J., Schäfer, H., Bötzel, K.,
… , Voges, J. (2006). A randomized trial of deep-brain stimulation for Parkinson’s
disease. New England Journal of Medicine, 355(9), 896–908.
Fava, M. (2003). Diagnosis and definition of treatment-resistant depression. Biological
Psychiatry, 53(8), 649–659.
Figee, M., Luigjes, J., Smolders, R., Valencia-Alfonso, C.-E., van Wingen, G., de
Kwaasteniet, B., … , Denys, D. (2013). Deep brain stimulation restores frontostriatal network activity in obsessive-compulsive disorder. Nature Neuroscience, 16(4),
386–387.
Gabriels, L., Cosyns, P., Nuttin, B., Demeulemeester, H., & Gybels, J. (2003). Deep
brain stimulation for treatment-refractory obsessive-compulsive disorder: Psychopathological and neuropsychological outcome in three cases. Acta Psychiatrica
Scandinavica, 107(4), 275–282.
Gazzaley, A., & Nobre, A. C. (2012). Top-down modulation: Bridging selective attention and working memory. Trends in Cognitive Sciences, 16(2), 129–135.
Greenberg, B. D., Gabriels, L. A., Malone, D. A., Rezai, A. R., Friehs, G. M., Okun,
M. S., … , Nuttin, B. J. (2010). Deep brain stimulation of the ventral internal capsule/ventral striatum for obsessive-compulsive disorder: Worldwide experience.
Molecular Psychiatry, 15(1), 64–79.
Hamilton, J. P., Etkin, A., Furman, D. J., Lemus, M. G., Johnson, R. F., & Gotlib, I. H.
(2012). Functional neuroimaging of major depressive disorder: A meta-analysis
and new integration of base line activation and neural response data. American
Journal of Psychiatry, 169(7), 693–703.
Hassler, R., Riechert, T., Mundinger, F., Umbach, W., & Ganglberger, J. A. (1960).
Physiological observations in stereotaxic operations in extrapyramidal motor disturbances. Brain, 83, 337–350.
Insel, T. R. (2014). The NIMH Research Domain Criteria (RDoC) Project: Precision
medicine for psychiatry. American Journal of Psychiatry, 171(4), 395–397.
Insel, T. R., & Wang, P. S. (2010). Rethinking mental illness. JAMA, 303(19), 1970–1971.
Kaur, N., Chou, T., Corse, A. K., Arulpragasam, A. R., Deckersbach, T., & Evans, K.
C. (2013). Deep brain stimulation for treatment-resistant depression. Psychiatric
Annals, 43(8), 358–365.
Kim, M. K., Kim, M., Oh, E., & Kim, S. P. (2013). A review on the computational
methods for emotional state estimation from the human EEG. Computational and
Mathematical Methods in Medicine, 2013, 573734.
Koran, L. M., Hanna, G. L., Hollander, E., Nestadt, G., & Simpson, H. B. (2007). Practice guideline for the treatment of patients with obsessive-compulsive disorder.
American Journal of Psychiatry, 164(7 Suppl), 5–53.
Kronig, M. H., Apter, J., Asnis, G., Bystritsky, A., Curtis, G., Ferquson, J., … , Du
Pont, I. J. (1999). Placebo-controlled, multicenter study of sertraline treatment
for obsessive-compulsive disorder. Journal of Clinical Psychopharmacology, 19(2),
172–176.
�14
EMERGING TRENDS IN THE SOCIAL AND BEHAVIORAL SCIENCES
Malone, D. (2010). Use of deep brain stimulation in treatment-resistant depression.
Cleveland Clinic Journal of Medicine, 77(Suppl. 3), 77–80.
Malone, D. A., Jr., Dougherty, D. D., Rezai, A. R., Carpenter, L. L., Friehs, G. M.,
Eskandar, E. N., … , Greenberg, B. D., (2009). Deep brain stimulation of the ventral
capsule/ventral striatum for treatment-resistant depression. Biological Psychiatry,
65(4), 267–275.
Manschreck, T. C., & Boshes, R. A. (2007). The CATIE schizophrenia trial: Results,
impact, controversy. Harvard Review of Psychiatry, 15(5), 245–258.
Marin, M. F., Camprodon, M. D., Dougherty, D. D., & Milad, M. R. (2014).
Device-based brain stimulation to augment fear extinction: implications for PTSD
treatment and beyond. Depression and Anxiety, 31(4), 269–278.
Mayberg, H. S. (2009). Targeted electrode-based modulation of neural circuits for
depression. Journal of Clinical Investigation, 119(4), 717–725.
Mayberg, H. S., Lozano, A. M., Voon, V., McNeely, H. E., Seminowicz, D., Hamani, C.,
… , Kennedy, S. H. (2005). Deep brain stimulation for treatment-resistant depression. Neuron, 45(5), 651–660.
McIntyre, C. C., & Foutz, T. J. (2013). Computational modeling of deep brain stimulation. Handbook of Clinical Neurology, 116, 55–61.
McIntyre, C. C., Grill, W. M., Sherman, D. L., & Thakor, N. V. (2004). Cellular effects of
deep brain stimulation: Model-based analysis of activation and inhibition. Journal
of Neurophysiology, 91(4), 1457–1469.
Milad, M. R., Orr, S. P., Lasko, N. B., Chang, Y., Rauch, S. L., & Pitman, R. K. (2008).
Presence and acquired origin of reduced recall for fear extinction in PTSD: results
of a twin study. Journal of Psychiatric Research, 42(7), 515–520.
Milad, M. R., & Rauch, S. L. (2007). The role of the orbitofrontal cortex in anxiety
disorders. Annals of the New York Academy of Sciences, 1121, 546–561.
Milad, M. R., Wright, C. I., Orr, S. P., Pitman, R. K., Quirk, G. J., & Rauch, S. L. (2007).
Recall of fear extinction in humans activates the ventromedial prefrontal cortex
and hippocampus in concert. Biological Psychiatry, 62(5), 446–454.
Mueller J., Skoqseid, I., Benecke, R., Kupsch, A., Trottenberg, T., Poewe, W., … ,
Volkmann, J. (2008). Pallidal deep brain stimulation improves quality of life in
segmental and generalized dystonia: results from a prospective, randomized
sham-controlled trial. Movement Disorders, 23(1), 131–134.
Nuttin, B., Cosyns, P., Demeulemeester, H., Gybels, J., & Meyerson, B. (1999).
Electrical stimulation in anterior limbs of internal capsules in patients with
obsessive-compulsive disorder. Lancet, 354(9189), 1526.
Price, J. L., & Drevets, W. C. (2012). Neural circuits underlying the pathophysiology
of mood disorders. Trends in Cognitive Sciences, 16(1), 61–71.
Riva-Posse, P., Choi, K. S., Holtzheimer, P. E., Mclntyre, C. C., Gross, R. E.,
Chaturvedi, A., … , Mayberg, H. S. (2014). Defining critical white matter pathways mediating successful subcallosal cingulate deep brain stimulation for
treatment-resistant sepression. Biological Psychiatry (Epub ahead of print).
Sitaram, R., Lee, S., Ruiz, S., Rana, M., Veit, R., & Birbaumer, N. (2011). Real-time
support vector classification and feedback of multiple emotional brain states. Neuroimage, 56(2), 753–765.
�Deep Brain Stimulation for Psychiatric Disorders
15
Warden, D., Rush, A. J., Trivedi, M. H., Fava, M., & Wisniewski, S. R. (2007). The
STAR*D project results: A comprehensive review of findings. Current Psychiatry
Reports, 9(6), 449–459.
Widge, A. S., Dougherty, D. D., & Moritz, C. T. (2014). Affective brain-computer
interfaces as enabling technology for responsive psychiatric stimulation.
Brain-Computer Interfaces, 1(2), 126–136.
Widge, A. S., & Moritz, C. T. (2014). Pre-frontal control of closed-loop limbic neurostimulation by rodents using a brain-computer interface. Journal of Neural Engineering, 11(2), 024001.
ALIK S. WIDGE SHORT BIOGRAPHY
Alik S. Widge is the Director of the Translational NeuroEngineering Laboratory and a clinician in the Division of Neurotherapeutics at Massachusetts
General Hospital. He completed combined MD/PhD training at the University of Pittsburgh and Carnegie Mellon University, followed by psychiatry
residency at the University of Washington. He remains a member of the joint
UW-MIT Center for Sensorimotor Neural Engineering. Dr. Widge’s research
centers around “closed loop” brain stimulators that sense and respond to
ongoing brain activity. He produced the first working demonstration of such
a stimulator in the psychiatric domain, and is now engaged in research to
bring this technology into human use.
http://scholar.harvard.edu/awidge/
AMANDA R. ARULPRAGASAM SHORT BIOGRAPHY
Amanda R. Arulpragasam is a clinical research coordinator within the
Division of Neurotherapeutics at the Massachusetts General Hospital. Her
research focuses on the use of neuroimaging techniques to better understand
psychiatric disorders as well as the mechanism of action of treatment
interventions (such as DBS).
THILO DECKERSBACH SHORT BIOGRAPHY
Thilo Deckersbach, PhD is an Associate Professor of Psychology at Harvard
Medical School. He serves as the Director of Research in the Division of Neurotherapeutics, the Director of Psychology in the Bipolar Clinic and Research
Program and as the Director of the MGH Graduate Student Division at at the
Massachusetts General Hospital in Boston. Dr. Deckersbach’s research has
been supported by the National Institute of Mental Health, NARSAD, TSA,
OCF, and DBDAT. He has published over 95 peer-reviewed papers and book
�16
EMERGING TRENDS IN THE SOCIAL AND BEHAVIORAL SCIENCES
chapters. His functional neuroimaging research (fMRI and PET) focuses on
the interaction of cognitive and emotional processes in bipolar disorder.
DARIN D. DOUGHERTY SHORT BIOGRAPHY
Dr. Darin D. Dougherty is the Director of the Neurotherapeutics Division in
the Department of Psychiatry at MGH, the Director of the Mood Disorders
Section of the Massachusetts General Hospital Psychiatric Neuroimaging
Group, and the Associate Director of the Massachusetts General Hospital
Psychiatric Neuroimaging Group. Dr. Dougherty is also the Director of Medical Education at the Massachusetts General Hospital Obsessive-Compulsive
Disorder Institute and the Co-Director of the Massachusetts General Hospital Trichotillomania Clinic. Additionally, Dr. Dougherty is an Associate
Professor of Psychiatry at Harvard Medical School, a Clinical Associate at
Massachusetts General Hospital and a Visiting Scientist at Massachusetts
Institute of Technology.Dr. Dougherty currently serves on the scientific advisory board for both the Anxiety Disorders Association of America and the
Obsessive Compulsive Foundation. He serves on the Massachusetts General
Hospital Psychiatric Neurosurgery Committee. He also serves on many
editorial boards and award committees. He has given over a hundred invited
lectures and presentations, and is a current member of many professional
societies. In 2003 Dr. Dougherty was awarded a NARSAD Young Investigator Award. In 2005 he was named one of the Future Leaders in Psychiatry.
Dr. Dougherty has co-authored over 100 original articles in peer-reviewed
journals, book chapters, and review articles, and has co-edited two books
on neuroimaging. Currently Dr. Dougherty is the Principal Investigator
or co-Principal Investigator on several government and industry funded
studies investigating neuroimaging and medication and neurosurgery treatments of OCD and mood disorders.Dr. Dougherty received his MD from the
University of Illinois and completed his residency in general psychiatry at
Massachusetts General Hospital. He is a graduate of the Clinical Investigator
Training Program at Harvard Medical School and Massachusetts Institute of
Technology. Dr. Dougherty’s research interests include neuroimaging, neurobiology, psychopharmacology, and neurotherapeutic (device and/or surgical) interventions for the treatment of treatment-refractory psychiatric illness.
RELATED ESSAYS
Positive Emotion Disturbance (Psychology), June Gruber and John Purcell
What Is Neuroticism, and Can We Treat It? (Psychology), Amantia Ametaj
et al.
Peers and Adolescent Risk Taking (Psychology), Jason Chein
�Deep Brain Stimulation for Psychiatric Disorders
17
Delusions (Psychology), Max Coltheart
Misinformation and How to Correct It (Psychology), John Cook et al.
Problems Attract Problems: A Network Perspective on Mental Disorders
(Psychology), Angélique Cramer and Denny Borsboom
Controlling the Influence of Stereotypes on One’s Thoughts (Psychology),
Patrick S. Forscher and Patricia G. Devine
Depression (Psychology), Ian H. Gotlib and Daniella J. Furman
Mental Imagery in Psychological Disorders (Psychology), Emily A. Holmes
et al.
Normal Negative Emotions and Mental Disorders (Sociology), Allan V.
Horwitz
Dissociation and Dissociative Identity Disorder (DID) (Psychology), Rafaële
J. C. Huntjens and Martin J. Dorahy
Computer Technology and Children’s Mental Health (Psychology), Philip C.
Kendall et al.
Cultural Neuroscience: Connecting Culture, Brain, and Genes (Psychology),
Shinobu Kitayama and Sarah Huff
Mechanisms of Fear Reducation (Psychology), Cynthia L. Lancaster and
Marie-H. Monfils
Disorders of Consciousness (Psychology), Martin M. Monti
Cognitive Bias Modification in Mental (Psychology), Meg M. Reuland et al.
Clarifying the Nature and Structure of Personality Disorder (Psychology),
Takakuni Suzuki and Douglas B. Samuel
A Gene-Environment Approach to Understanding Youth Antisocial Behavior (Psychology), Rebecca Waller et al.
Rumination (Psychology), Edward R. Watkins
�
-
Deep Brain Stimulation for
Psychiatric Disorders
ALIK S. WIDGE, AMANDA R. ARULPRAGASAM,
THILO DECKERSBACH, and DARIN D. DOUGHERTY
Abstract
In this monograph, we briefly review the rationale for deep brain stimulation (DBS)
for psychiatric illness, beginning with current noninvasive treatment options and
progressing to the evolution and success of DBS as a therapy. This discussion will
focus on obsessive-compulsive disorder (OCD) and major depressive disorder
(MDD) particularly, as these are the only two diagnoses that have been subjected to
adequately controlled DBS trials to date. The majority of the essay then describes
the significant limitations that DBS is currently facing and emerging approaches
to address them. This will lead into a discussion of new technologies such as
patient-specific modeling of electric fields and closed-loop DBS systems and how
we can best utilize these to increase our understanding of DBS and the overall
efficacy of this novel therapy.
INTRODUCTION: THE RATIONALE FOR DBS IN PSYCHIATRY
The most common treatments for psychiatric disorders are medications and
psychotherapy. However, several large scale studies have shown that even
best-evidence treatment fails to help a substantial fraction of patients (Manschreck & Boshes, 2007; Warden, Rush, Trivedi, Fava, & Wisniewski, 2007).
Obsessive-compulsive disorder (OCD) is a chronic psychiatric disorder
that affects approximately 3% of the world’s population. Presently, first-line
treatment options include cognitive-behavioral therapy and medications
such as serotonergic reuptake inhibitors (SSRIs) (Koran, Hanna, Hollander,
Nestadt, & Simpson, 2007). Approximately one third of patients may not
experience substantial benefit despite receiving both medication and behavioral therapy (Kronig et al., 1999). Major depressive disorder (MDD) is one of
the leading causes of disability in the world and affects approximately 14.8
million American adults with a lifetime prevalence rate of 19.2% (Bromet
et al., 2011). It is estimated that 50–60% of these patients fail to fully respond
to an antidepressant in which adequate dosing and duration have occurred
Emerging Trends in the Social and Behavioral Sciences. Edited by Robert Scott and Stephen Kosslyn.
© 2015 John Wiley & Sons, Inc. ISBN 978-1-118-90077-2.
1
�2
EMERGING TRENDS IN THE SOCIAL AND BEHAVIORAL SCIENCES
(Fava, 2003). For depression, other options such as electro-convulsive
therapy (ECT) or transcranial magnetic stimulation (TMS) also exist. For
OCD, once medications and intensive therapy have failed, patients have few
further treatment options.
During the last 10–15 years, we have witnessed a major paradigm shift
in the conceptualization of psychiatric disorders (Mayberg, 2009). Basic
research has significantly advanced our understanding of the anatomy
and physiology of brain networks and their mechanisms for processing
cognition, behavior, and emotion. An example of such a circuit can be shown
in Figures 1 and 2. The advancement of our knowledge in neural circuitry
has had a major impact by transforming our understanding of psychiatric
pathophysiology, and has also set the stage for new treatment modalities
that directly modulate disease-relevant circuits (Arulpragasam et al., 2013).
One such treatment that has been shown to modulate maladaptive circuitry
is DBS. DBS is a nonlesion-based, reversible neuromodulation therapy. DBS
Exteroception
-Attention
-Appraisal
-Action
Mood regulation
-Attention
-Appraisal
-Action
mFC
PFC
PMC
ParC
MCC
dpHC
PCC
VS-CDT
dmTH
AMYG
MB-VTA
pACC
mOFC
SCC
AntIns
Mood monitoring
-Novelty
-Salience
-Habit
va-HC
HTH
BS
Interoception
-Drive states
-Autonomic function
-Circadian rhythms
Figure 1 The functional neurocircuitry of obsessive-compulsive disorder (OCD)
as described by Corse et al. 2013. Hypoactivity of the cortico-striatal-thalamiccortical (CSTC) loop (between the OFC and striatum) or hyperactivity of the
corticothalamic (CT) loop (between the OFC/PFC and the thalamus) may result in
OCD symptoms. ACC = anterior cingulate cortex; OFC = orbitofrontal cortex;
PFC = prefrontal cortex.
�Deep Brain Stimulation for Psychiatric Disorders
3
Negative
feedback
loop (−)
Striatum
Thalamus
CSTC
CT loop (+)
OFC
PFC
Frontal
cortex
ACC
Limbic
system
Figure 2 Circuit model of MDD. Adapted from Mayberg, 2009. Regions with
known anatomical interconnections that show consistent changes across
converging imaging experiments form the basis of this model. Regions are
grouped into four main compartments, reflecting general behavioral dimensions of
MDD and regional targets of various antidepressant treatments. Regions within a
compartment all have strong anatomical connections to one another. Black arrows
identify cross-compartment anatomical connections. Solid colored arrows identify
putative connections between compartments mediating a specific treatment.
AntIns = anterior insula; AMYG = amygdala; BS = brainstem; dmTH = dorsomedial
thalamus; dpHC = dorsal-posterior hippocampus; HTH = hypothalamus;
MB-VTA = midbrain-ventral tegmental area; MCC = medial cingulate cortex;
mFC = medial frontal cortex; mOFC = medial orbital frontal cortex; pACC = the
perigenual area of the anterior cingulate cortex; ParC = parietal cortex; PCC =
posterior cingulate cortex; PFC = prefrontal cortex; PMC = premotor cortex;
va-HC = ventral-anterior hippocampus; SCC = subcallosal cingulate; VS-CDT =
ventral striatum-caudate.
involves surgically implanting electrodes at specific target locations within
the brain and delivering electrical pulses of adjustable frequency and
intensity through those electrodes (Corse et al., 2013). In the early 1960s, it
was shown that electrical stimulation of the ventrolateral thalamus could
alleviate tremor (Hassler, Riechert, Mundinger, Umbach, & Ganglberger,
1960) and in the early 1990s, DBS was further developed for the treatment
of essential tremor and Parkinson’s disease (PD) (Benabid et al., 1991). Since
then, the safety and efficacy of DBS for movement disorders such as PD,
essential tremor and extrapyramidal dyskinesia has been repeatedly demonstrated in rigorous clinical trials (Deuschl et al., 2006; Mueller et al., 2008).
The FDA approved the use of DBS for PD in 2002, and since then, over 70,000
patients have undergone DBS for this specific indication (Bronstein et al.,
2011).
�4
EMERGING TRENDS IN THE SOCIAL AND BEHAVIORAL SCIENCES
The success of DBS in modulating pathological circuitry in movement disorders suggests that it may be a viable option for treating disorders that result
from maladaptive changes in brain circuits leading to pathological processing of affective and behavioral information, in patients who do not respond to
medication, psychotherapy, or other less invasive treatment modalities. This
definition of “maladaptive changes in brain circuits” encompasses most, if
not all, psychiatric disorders. As such, exploration and investigation of the
potential benefits of DBS in refractory psychiatric illness is justified.
FOUNDATIONAL AND CUTTING-EDGE WORK: STATE OF THE
ART OF DBS IN PSYCHIATRY
DBS was first investigated by Nuttin and colleagues in 1999 (Nuttin, Cosyns,
Demeulemeester, Gybels, & Meyerson, 1999) in patients with refractory
OCD, in what was also the first ever recorded case series of DBS performed
specifically for a psychiatric indication. This early report prompted ongoing
investigations, which continued to demonstrate similar, successful results
(Abelson et al., 2005; Gabriels, Cosyns, Nuttin, Demeulemeester, & Gybels,
2003). The internal capsule site most commonly studied for OCD is derived
from the location for ablative procedures for treatment-resistant OCD and
anterior capsulotomy (Corse et al., 2013) DBS at this site was expected
to modulate of circuitry specifically implicated in the pathophysiology
of OCD.
Over time, the target moved to a location slightly more posterior than a
traditional capsulotomy. This new location is thought to be the junction of
the anterior commissure, internal capsule, and striatum (Greenberg et al.,
2010), and thus is called the “ventral capsule/ventral striatum” (VC/VS).
At this target, the mean improvement in Yale-Brown Obsessive-Compulsive
Scale (YBOCS) score was 38%, from 34 to 21 (Greenberg et al., 2010) Depression also improved, with a mean drop of 43% in Hamilton Depression Rating Scale (HDRS) and 50% of patients meeting criteria for depressive remission (HDRS < 7) at their last follow-up visit (Kaur et al., 2013) These positive
results led to the US Food and Drug Administration approving (on a limited
basis) DBS for treatment-resistant OCD at the VC/VS target in 2009 (Corse
et al., 2013). This was the first and remains the only approval for use of DBS
for a refractory psychiatric illness in nonresearch practice.
Intriguingly, DBS at VC/VS seemed to also alleviate comorbid depression.
Thus, Malone et al. (2009) conducted the first VC/VS DBS open-label, multicenter trial for treatment resistant depression (TRD) at three collaborating
clinical sites: the Cleveland Clinic, Butler Hospital/Brown Medical School,
and the Massachusetts General Hospital. This pilot study demonstrated a
40% MDD remission rate. An expanded cohort reported in 2010 showed
�Deep Brain Stimulation for Psychiatric Disorders
5
similar results, with a 71% response rate at the last follow-up (Malone,
2010). Surprisingly, a multi-center randomized trial conducted following
these open-label reports did not reach significance and was stopped because
of interim analyses [D. Dougherty, unpublished results]. In parallel, the
Mayberg-Lozano group at the University of Toronto and Emory University
conducted a very similar trial at a different target, the subgenual cingulate
gyrus (Cg25) (Mayberg et al., 2005). That target was rationally selected based
on over a decade of neuro-imaging studies, and had also shown positive
open-label results (Mayberg, 2009). Despite this, the Cg25 trial also failed to
achieve its primary endpoint.
THE CRITICAL NEED: GREATER UNDERSTANDING FOR TRULY
EFFECTIVE DBS
These previous studies demonstrated the promise of DBS in the field of neuropsychiatry, but also highlighted its current shortcomings. It is clear that the
research community has not yet identified the anatomic targets or electrical
parameters that can deliver on that promise. There is much more we need to
know and investigate to optimize DBS.
First, a better understanding of how DBS works and how this stimulation
actually affects individual neurons and larger brain circuitry would enable
more rational therapeutic design. As described above, most DBS targeting is
based on anatomy—on regions that are hyper-active during brain imaging or
where neurosurgeons have successfully treated disease by lesioning tissue.
The clinical trials have shown us that it is not enough to have the electrode
in the right part of the brain. Instead, we need to understand what exactly
the electrical stimulation is doing to the neurons in that tissue, and how the
signal might be propagating through the complex circuitry of the brain.
Secondly, state of the art DBS devices are open loop systems. Present DBS
systems deliver energy continuously at a pre-programmed frequency and
amplitude, with parameter adjustments only occurring during relatively
infrequent clinical programming visits (roughly every 3 months) (Widge,
Dougherty, & Moritz, 2014). DBS needs to progress to becoming “closed
loop”—to being able to monitor its efficacy in real-time and to automatically
adjust stimulation in response to that monitoring. While these systems have
demonstrated therapeutic benefit, they incorrectly assume that psychiatric
symptoms are static. Clinically symptoms of many disorders vary day to
day or moment to moment. Systems that can monitor and respond to these
changing symptoms may have greater tolerability or better response rates.
Lastly, psychiatric diagnoses may not map well to brain entities that can
be targeted through DBS. The categorical nature of psychiatric diagnosis
means that two patients with the same disorder may have very little overlap
�6
EMERGING TRENDS IN THE SOCIAL AND BEHAVIORAL SCIENCES
in symptoms. Further, most patients with severe psychiatric disorders have
co-occurring diagnoses. Symptoms overlap across diagnostic boundaries.
Therefore, a trans-diagnostic approach that focuses on underlying functional
dimensions may improve the mapping between symptoms and neural activity. The remaining portion of this essay will expand on these three points
and provide insight and ideas as to how we believe the field can move
forward.
EMERGING TREND: DEEPER UNDERSTANDING OF THE NEURAL
MECHANISMS OF DBS
To improve the efficacy of DBS, we must better understand its underlying
mechanism of action. Previously, it was thought that DBS merely simulated
the effect of lesioning tissue (Bronstein et al., 2011). However, we now believe
the mechanism to be much more complicated.
While the exact mechanism of action remains unknown, there are several
current theories. McIntyre, Grill, Sherman, & Thakor (2004) noted that several
experimental studies have produced contradictory results, showing inhibition of activity in the stimulated target, but increased inputs to projection
nuclei. To explain these seemingly opposite findings, they studied stimulation using a computational model that incorporated representations of a
clinical DBS electrode and a thalamocortical relay neuron.
They found that the response of the neuron to DBS was primarily dependent on the position and orientation of the axon with respect to the electrode
and the parameters of stimulation (McIntyre et al., 2004). Intracellular stimulation applied within the cell body generated action potentials that were
transmitted down the axon with the same stimulus frequency. However,
extracellular DBS (the actual modality used clinically) resulted in independent firing of the cell body and axon at high stimulation frequencies. This
suggests that during high frequency stimulation, cell body activity may be
decoupled from axonal activity, and a single neuron may simultaneously be
inhibited at its soma (where it receives input from other cells) and excited in
its axon (its output to downstream cells) (McIntyre et al., 2004). This creates
an “information blockade”—there is no meaningful relationship between
the firing of cells upstream of the stimulated neuron and the output that the
neuron sends to its targets. It is no longer able to perform a computational
function. Depending on where the stimulated neuron falls in a brain circuit,
this could act as a lesion of the tissue, or it could act as though the stimulated
nucleus were hyperactive. Detailed computer modeling of DBS is continuing
to emerge as a powerful technique to enhance our understanding of the
effects of DBS and to create a virtual test platform for novel stimulation
strategies (McIntyre & Foutz, 2013). The next step will be expanding this
�Deep Brain Stimulation for Psychiatric Disorders
7
modeling to a wide range of tissues and electrode configurations, a task
which will be mathematically and computationally difficult.
Alongside computational modeling, there is growing interest in recording while using DBS in patients to better understand the underlying neural
mechanism of DBS. Figee et al. (2013) used functional magnetic resonance
imaging (fMRI) and electroencephalography (EEG) to investigate nucleus
accumbens (NAc) DBS in 16 OCD patients. By alternating between a DBS
ON and DBS OFF state, they were able to measure differences in NAc activity
as a result of stimulation. During DBS OFF, the NAc activity in patients was
lower than in controls, whereas during DBS ON, patients had similar NAc
activity as healthy controls (Widge et al., 2014). This suggests that DBS has the
capacity to normalize NAc activity—the exact opposite of the classical “lesion” hypothesis. They also found that DBS targeted at the NAc within OCD
patients reduced excessive connectivity between the NAc and prefrontal cortex (PFC) and also attenuated the increase in low-frequency PFC activity
elicited by symptom provocation (Figee et al., 2013). Thus, there is support
for a theory that DBS may act in psychiatric illness not by modulating a single brain area, but instead by altering connectivity patterns between multiple
areas.
Using a similar method of alternating between DBS ON and DBS OFF
states, Cavanagh et al. (2011) measured changes in subthalamic nucleus
(STN) activity through EEG in patients with STN DBS for PD (Cavanagh
et al., 2011). They used a reinforcement learning and choice conflict task in
which participants were asked to select between novel stimulus combinations involving low (win–lose) or high (win–win and lose–lose) decision
conflict (Cavanagh et al., 2011). They found that during the DBS ON condition, patients responded faster when making suboptimal (poorer) choice
than when making optimal choices. There was no difference in response
time during the DBS OFF condition (Cavanagh et al., 2011). In other words,
DBS of this site caused a subtle psychiatric symptom—a tendency toward
premature responding that drove them to make poor, impulsive choices.
EEG recordings in the medial PFC (mPFC) predicted slower response times
during high-conflict trials in healthy control participants and patients in
the DBS OFF condition, but not in the DBS ON state (Cavanagh et al.,
2011). Here again, it appears that multiple structures (at least mPFC and
STN) are communicating in a network to produce a cognitive phenomenon
(decision-making), and DBS can alter that communication to produce
behavior change.
As the available base of patients with DBS at different brain sites increases,
studies such as these will become increasingly feasible. Furthermore,
advances in imaging and recording technology, along with signal processing, will make it easier for neuroscientists to interpret the findings of these
�8
EMERGING TRENDS IN THE SOCIAL AND BEHAVIORAL SCIENCES
studies. It can also be expected that there will be more and better behavioral
tasks developed, which will help us understand how DBS of each brain
region subtly alters patients’ behavior. The clinical use of DBS according to
anatomic targeting rules will help us produce the neuroscientific data that
will lead to much more rational targeting and programming.
A closely related trend is patient-specific modeling of the spread of the
electric field and its effects on cells and circuits. Riva-Posse et al. (2014) used
diffusion tensor imaging (DTI, a method of mapping connections in the
brain) to model white matter connections and identify the pathways that
govern DBS response for depression. In this study, preoperative MRI data,
including DTI, were acquired in 16 TRD patients. The patients then received
DBS implants at the subcallosal cingulate (Cg25) target. Postoperatively,
computerized tomography was used to locate DBS contacts. The activation
volume around the contacts used for stimulation was then modeled for each
patient and patient-specific tract maps were calculated (Riva-Posse et al.,
2014). The patients were then clinically assessed for therapeutic response at
6 months and 2 years post implant. DBS responders at 6 months (n = 6) and
2 years (n = 12) shared bilateral pathways from their individual activation
volumes to the medial frontal cortex, rostral and dorsal cingulate cortex, and
subcortical nuclei. Nonresponders, on the other hand, did not show these
connections consistently (Riva-Posse et al., 2014). This is a preliminary, but
exciting result—it suggests that it may be possible to define, for each individual patient, the exact anatomic coordinates that would place their DBS at a
“hub” connected to a wide variety of brain areas. If the network-modulation
hypothesis is correct, DBS at a highly-connected hub should be much more
effective. Future years will hopefully show us prospective tests of this
method.
EMERGING TREND: CLOSING THE LOOP
Psychiatric symptoms are not static. Symptoms flare and subside, on a
timescale of minutes to hours. Existing DBS strategies have been unable
to effectively treat such fluctuations, because they occur on significantly
shorter timescales than the relatively infrequent clinical programming
visits. It has been proposed that the stimulator could become “closed
loop”—it could actively monitor the patient’s current emotional state, then
adjust stimulation to compensate. Ideally, stimulation could go from the
present paradigm continuous operation (always on, fixed parameters) to
an intermittent, responsive mode (on only when the patient needs it, with
dynamically adjusting paramters) (Widge et al., 2014). In many ways, this
is the same problem as brain-computer interfaces (BCIs), a technology
currently used to treat paralysis by “decoding” movement commands
�Deep Brain Stimulation for Psychiatric Disorders
9
from the motor cortex. In a psychiatric DBS, the BCI would continuously
monitor emotional state and adjust stimulation parameters to maintain the
patient in an optimal range (Widge et al., 2014). The emotional state signals
are already established to occur within the brain, particularly within the
PFC, which specifically serves emotional regulation functions (Hamilton
et al., 2012). A responsive system would assume some of that regulatory
function to compensate for circuits that have become either dysfunctional
or hypofunctional. Moreover, it would deliver electrical stimulation that is
appropriate to the patient’s immediate need. This would in turn reduce the
side effects associated with over-stimulation, alleviate residual symptoms
related to under-stimulation, and optimize power consumption, leading to
slower battery depletion (Widge et al., 2014). Major funding agencies in the
United States have committed to developing these closed-loop systems,1 and
DBS manufacturers have already released hardware that could implement
them (Afshar et al., 2013).
The development of closed-loop emotional DBS is a promising new
approach but it has been hindered by a lack of feasible electrical biomarkers.
That is, it is unknown what the electrical signature of psychiatric illness
or remission looks like within the brain. Until we know what the DBS
should sense, it is difficult to build a closed-loop controller that decodes
critical psychiatric information from neural firing. fMRI can provide insights
into activity across the whole brain (Sitaram et al., 2011), however, most
fMRI sequences are not fully compatible with DBS implanted devices and
thus, unfortunately, cannot be utilized. Second, decoding modalities that
support continuous recording may not function properly in the presence of
psychiatric disorders (Widge et al., 2014). EEG has been a very successful
method for noninvasive emotion decoding in human volunteers (Kim, Kim,
Oh, & Kim, 2013). However, all successful EEG emotion decoding has only
been shown in healthy control participants. Patients with mental illness,
by definition, do not have normal neural circuits or activation. Therefore,
measures that accurately classify healthy controls may not transfer over to
this population. Furthermore, there is a consensus that clinical diagnoses
oftentimes contain multiple neurologic entities and that the same clinical
phenotype might arise from diametrically opposite changes in the brain
(Cuthbert & Insel, 2013). This could present a potential challenge for clinical
translation of existing emotional decoders (Widge et al., 2014). Third, even
if BCIs are able to function in the presence of clinical symptoms, they
may not be able to adequately distinguish pathologic states from normal
states (Widge et al., 2014). Psychiatric disorders are marked by extremes
of emotions that are normally occurring in everyday life. The difference
1. http://www.technologyreview.com/news/527561/military-funds-brain-computer-interfaces-tocontrol-feelings/. [cited 2014 Jun 14].
�10
EMERGING TRENDS IN THE SOCIAL AND BEHAVIORAL SCIENCES
is not severity or type, but rather its context and appropriateness in a
given situation. In post-traumatic stress disorder (PTSD) for example,
patients may overgeneralize from a fearful event and later experience high
vigilance and arousal in contexts that are objectively safe. The question is
differentiation—can we tell whether a patient is having a PTSD flashback
(where the BCI-DBS system should intervene to reduce his/her fear) or
watching a thrilling movie (where the BCI-DBS should allow the patient
to enjoy this normal and healthy human experience)? A system that fails
to distinguish could actually be more harmful than the symptoms it seeks to
treat.
The search for those biomarkers will be a critical trend in DBS research
in the coming decade. However, equally important is the question of
whether we might be able to create a closed-loop DBS while foregoing
biomarkers entirely. Recent demonstrations have suggested a completely
new approach—direct volitional control of the neurostimulator. In such a
device, a patient would sense that current stimulation parameters are not
well matched to his/her clinical needs, then directly communicate this to
the stimulation by deliberately modulating specific aspects of brain activity
(Widge et al., 2014). This is even more directly a use of the BCI technologies
described above—those technologies were developed for exactly this kind
of “intention decoding”. In this scenario, we would not need to worry
about the BCI’s ability to classify an emotion as pathologic vs. healthy—the
patient would “tell” the stimulator directly whether the current emotional
experience was desirable or undesirable. This could occur in real-time,
changing stimulation moment-to-moment to track experienced symptoms,
rather than waiting weeks between programming visits. Heterogeneity of
biomarkers would also be a moot point – the only important variable would
be the patient’s own intention to receive mood-altering stimulation (Widge
et al., 2014). A proof-of-concept demonstration of this approach has recently
occurred in an animal model. Rats have used such a system to directly
trigger stimulation to the medial forebrain bundle (MFB), a structure within
the reward pathway where electrical stimulation is known to be reinforcing
(Widge & Moritz, 2014). This volitional pathway to closed-loop DBS has
much work to be done before it becomes a clinical reality, but offers the
exciting possibility that patients could literally regain their capacity for
self-control.
EMERGING TREND: RATIONAL DESIGN AND TRIALS OF
PSYCHIATRIC NEUROTHERAPEUTICS
In discussing the potential for closed-loop systems, we have described the
present lack of identified, treatable neural biomarkers of DSM disorders. One
�Deep Brain Stimulation for Psychiatric Disorders
11
reason for this is that symptom-based psychiatric diagnoses may not be neurological entities (Cuthbert & Insel, 2013; Insel & Wang, 2010). That is, if a
single disorder/diagnosis can be achieved by a wide variety of symptom
clusters, it is reasonable to believe that those clusters might be produced
by a variety of underlying problems in brain structures and circuits. If this
is true, the failure to find a neurological basis of psychiatric illness is not
surprising—a search for specific brain dysfunction cannot lead to significant
findings if only a small subset of studied patients actually have that dysfunction. To produce a clearer picture of the mapping between symptoms and
neural activity, we likely need to move away from focusing on categorical
diagnoses which lead to extraneous overlap and instead focus on modeling,
targeting and treating the functional problems that underpin those diagnoses
(Cuthbert & Insel, 2013; Insel, 2014).
There are known correlates and behavioral tests for working memory (Gazzaley & Nobre, 2012), impulsivity (Bari & Robbins, 2013), emotion regulation
(Price & Drevets, 2012), and many other behaviors that cut across mental illnesses. Instead of treating heterogeneous disorders, one could develop tests
for those functional domains, and then target stimulation to domain-specific
symptoms and circuits. Doing so would address what is actually pathological
for each individual patient. Furthermore, moving to a domain-oriented diagnosis and treatment system would better leverage extensive animal work
in brain stimulation. Psychiatric treatment screening in animals is limited,
because there is no evidence that animal behavioral tests produce analogues
of human emotion. There is, however, proof for observable behavior changes
on standardized tests. A transdiagnostic approach would focus on what can
be precisely measured in both animals and humans, and could thus allow us
to treat real, quantifiable phenomena.
One such example for the application of this new approach is extinction
learning. There is a rapidly evolving literature on fear extinction and
the fear-safety learning network, which includes the ventromedial PFC,
amygdala and hippocampus (Marin, Camprodon, Dougherty, & Milad,
2014; Milad & Rauch, 2007; Milad et al., 2007). There is considerable overlap
between this fear extinction network and several brain regions associated
with symptom severity in psychiatric illnesses such as OCD, MDD and most
notably, PTSD (Marin et al., 2014; Milad et al., 2008). This suggests that if we
could work out a DBS that specifically targeted the fear network (leveraging
the emerging evidence on network effects of DBS), that single intervention
could be applicable to numerous mental disorders (Marin et al., 2014).
This transdiagnostic approach would face numerous hurdles. Most of
the existing scientific literature is disease/disorder oriented, making it
difficult to re-tool studies to address domains. Further, there would be
substantial regulatory hurdles—at least in the United States, devices are
�12
EMERGING TRENDS IN THE SOCIAL AND BEHAVIORAL SCIENCES
usually approved to treat specific diagnoses. Funding agencies have begun
to propose the transdiagnostic approach, (Insel, 2014) but it will be some
time before this idea is well adopted, let alone suitable for use in clinical
practice. Nevertheless, this represents the progression of psychiatry (and
interventional psychiatry in particular) into a genuinely rational field, and
is a trend to be encouraged.
CONCLUSIONS
DBS for psychiatric illness has had great promise, but has stumbled in
converting that promise to clinical reality. Much of that relates to a lack
of understanding—of the mechanisms of action, biomarkers of efficacious
treatment, and the appropriate selection of patients/impairments to be
treated with implantable devices. Numerous investigators are actively
researching solutions to these problems, and the next decade promises great
advances.
REFERENCES
Abelson, J. L., Curtis, G. C., Saqher, O., Albucher, R. C., Harrigan, M., Taylor, S. F., … ,
Giordani, B. (2005). Deep brain stimulation for refractory obsessive-compulsive
disorder. Biological Psychiatry, 57(5), 510–516.
Afshar, P., Khambhati, A., Stanslaski, S., Carlson, D., Jensen, R., Linde, D., … ,
Denison, T. (2013). A translational platform for prototyping closed-loop neuromodulation systems. Front Neural Circuits, 6: 117.
Arulpragasam, A. R., Chou, T., Kaur, N., Corse, A. K., Deckersbach, T., &
Camprodon, J. A. (2013). Future directions of deep brain stimulation: current disorders, new technologies. Psychiatric Annals, 43(8), 366–373.
Bari, A., & Robbins, T. W. (2013). Inhibition and impulsivity: Behavioral and neural
basis of response control. Progress in Neurobiology, 108, 44–79.
Benabid, A. L., Pollak, P., Gervason, C., Hoffmann, D., Gao, D. M., Hommel, M. … ,
de Rougeont, J. (1991). Long-term suppression of tremor by chronic stimulation of
the ventral intermediate thalamic nucleus. Lancet, 337(8738), 403–406.
Bromet, E., Andrade, L. H., Hwang, I., Sampson, N. A., Alonso, J., de Girolamo, G.,
… , Kessler, R. C. (2011). Cross-national epidemiology of DSM-IV major depressive
episode. BMC Medicine 9: 90.
Bronstein, J. M., Taqliati, M., Alterman, R. L., Lozano, A. M., Volkmann, J., Stefani,
A., … , DeLong, M. R. (2011). Deep brain stimulation for parkinson disease: An
expert consensus and review of key issues. Archives of Neurology, 68(2), 165.
Cavanagh, J. F., Wiecki, T. V., Cohen, M. X., Figueroa, C. M., Samantha, J., Sherman,
S. J., & Frank, M. J. (2011). Subthalamic nucleus stimulation reverses mediofrontal
influence over decision threshold. Nature Neuroscience, 14(11), 1462–1467.
Corse, A. K., Chou, T., Arulpragasam, A. R., Kaur, N., Deckersbach, T., & Cusin,
C. (2013). Deep brain stimulation for obsessive-compulsive disorder. Psychiatric
Annals, 43(8), 351–357.
�Deep Brain Stimulation for Psychiatric Disorders
13
Cuthbert, B. N., & Insel, T. R. (2013). Toward the future of psychiatric diagnosis: The
seven pillars of RDoC. BMC Medicine, 11, 126.
Deuschl, G., Schade-Brittinger, C., Krack, P., Volkmann, J., Schäfer, H., Bötzel, K.,
… , Voges, J. (2006). A randomized trial of deep-brain stimulation for Parkinson’s
disease. New England Journal of Medicine, 355(9), 896–908.
Fava, M. (2003). Diagnosis and definition of treatment-resistant depression. Biological
Psychiatry, 53(8), 649–659.
Figee, M., Luigjes, J., Smolders, R., Valencia-Alfonso, C.-E., van Wingen, G., de
Kwaasteniet, B., … , Denys, D. (2013). Deep brain stimulation restores frontostriatal network activity in obsessive-compulsive disorder. Nature Neuroscience, 16(4),
386–387.
Gabriels, L., Cosyns, P., Nuttin, B., Demeulemeester, H., & Gybels, J. (2003). Deep
brain stimulation for treatment-refractory obsessive-compulsive disorder: Psychopathological and neuropsychological outcome in three cases. Acta Psychiatrica
Scandinavica, 107(4), 275–282.
Gazzaley, A., & Nobre, A. C. (2012). Top-down modulation: Bridging selective attention and working memory. Trends in Cognitive Sciences, 16(2), 129–135.
Greenberg, B. D., Gabriels, L. A., Malone, D. A., Rezai, A. R., Friehs, G. M., Okun,
M. S., … , Nuttin, B. J. (2010). Deep brain stimulation of the ventral internal capsule/ventral striatum for obsessive-compulsive disorder: Worldwide experience.
Molecular Psychiatry, 15(1), 64–79.
Hamilton, J. P., Etkin, A., Furman, D. J., Lemus, M. G., Johnson, R. F., & Gotlib, I. H.
(2012). Functional neuroimaging of major depressive disorder: A meta-analysis
and new integration of base line activation and neural response data. American
Journal of Psychiatry, 169(7), 693–703.
Hassler, R., Riechert, T., Mundinger, F., Umbach, W., & Ganglberger, J. A. (1960).
Physiological observations in stereotaxic operations in extrapyramidal motor disturbances. Brain, 83, 337–350.
Insel, T. R. (2014). The NIMH Research Domain Criteria (RDoC) Project: Precision
medicine for psychiatry. American Journal of Psychiatry, 171(4), 395–397.
Insel, T. R., & Wang, P. S. (2010). Rethinking mental illness. JAMA, 303(19), 1970–1971.
Kaur, N., Chou, T., Corse, A. K., Arulpragasam, A. R., Deckersbach, T., & Evans, K.
C. (2013). Deep brain stimulation for treatment-resistant depression. Psychiatric
Annals, 43(8), 358–365.
Kim, M. K., Kim, M., Oh, E., & Kim, S. P. (2013). A review on the computational
methods for emotional state estimation from the human EEG. Computational and
Mathematical Methods in Medicine, 2013, 573734.
Koran, L. M., Hanna, G. L., Hollander, E., Nestadt, G., & Simpson, H. B. (2007). Practice guideline for the treatment of patients with obsessive-compulsive disorder.
American Journal of Psychiatry, 164(7 Suppl), 5–53.
Kronig, M. H., Apter, J., Asnis, G., Bystritsky, A., Curtis, G., Ferquson, J., … , Du
Pont, I. J. (1999). Placebo-controlled, multicenter study of sertraline treatment
for obsessive-compulsive disorder. Journal of Clinical Psychopharmacology, 19(2),
172–176.
�14
EMERGING TRENDS IN THE SOCIAL AND BEHAVIORAL SCIENCES
Malone, D. (2010). Use of deep brain stimulation in treatment-resistant depression.
Cleveland Clinic Journal of Medicine, 77(Suppl. 3), 77–80.
Malone, D. A., Jr., Dougherty, D. D., Rezai, A. R., Carpenter, L. L., Friehs, G. M.,
Eskandar, E. N., … , Greenberg, B. D., (2009). Deep brain stimulation of the ventral
capsule/ventral striatum for treatment-resistant depression. Biological Psychiatry,
65(4), 267–275.
Manschreck, T. C., & Boshes, R. A. (2007). The CATIE schizophrenia trial: Results,
impact, controversy. Harvard Review of Psychiatry, 15(5), 245–258.
Marin, M. F., Camprodon, M. D., Dougherty, D. D., & Milad, M. R. (2014).
Device-based brain stimulation to augment fear extinction: implications for PTSD
treatment and beyond. Depression and Anxiety, 31(4), 269–278.
Mayberg, H. S. (2009). Targeted electrode-based modulation of neural circuits for
depression. Journal of Clinical Investigation, 119(4), 717–725.
Mayberg, H. S., Lozano, A. M., Voon, V., McNeely, H. E., Seminowicz, D., Hamani, C.,
… , Kennedy, S. H. (2005). Deep brain stimulation for treatment-resistant depression. Neuron, 45(5), 651–660.
McIntyre, C. C., & Foutz, T. J. (2013). Computational modeling of deep brain stimulation. Handbook of Clinical Neurology, 116, 55–61.
McIntyre, C. C., Grill, W. M., Sherman, D. L., & Thakor, N. V. (2004). Cellular effects of
deep brain stimulation: Model-based analysis of activation and inhibition. Journal
of Neurophysiology, 91(4), 1457–1469.
Milad, M. R., Orr, S. P., Lasko, N. B., Chang, Y., Rauch, S. L., & Pitman, R. K. (2008).
Presence and acquired origin of reduced recall for fear extinction in PTSD: results
of a twin study. Journal of Psychiatric Research, 42(7), 515–520.
Milad, M. R., & Rauch, S. L. (2007). The role of the orbitofrontal cortex in anxiety
disorders. Annals of the New York Academy of Sciences, 1121, 546–561.
Milad, M. R., Wright, C. I., Orr, S. P., Pitman, R. K., Quirk, G. J., & Rauch, S. L. (2007).
Recall of fear extinction in humans activates the ventromedial prefrontal cortex
and hippocampus in concert. Biological Psychiatry, 62(5), 446–454.
Mueller J., Skoqseid, I., Benecke, R., Kupsch, A., Trottenberg, T., Poewe, W., … ,
Volkmann, J. (2008). Pallidal deep brain stimulation improves quality of life in
segmental and generalized dystonia: results from a prospective, randomized
sham-controlled trial. Movement Disorders, 23(1), 131–134.
Nuttin, B., Cosyns, P., Demeulemeester, H., Gybels, J., & Meyerson, B. (1999).
Electrical stimulation in anterior limbs of internal capsules in patients with
obsessive-compulsive disorder. Lancet, 354(9189), 1526.
Price, J. L., & Drevets, W. C. (2012). Neural circuits underlying the pathophysiology
of mood disorders. Trends in Cognitive Sciences, 16(1), 61–71.
Riva-Posse, P., Choi, K. S., Holtzheimer, P. E., Mclntyre, C. C., Gross, R. E.,
Chaturvedi, A., … , Mayberg, H. S. (2014). Defining critical white matter pathways mediating successful subcallosal cingulate deep brain stimulation for
treatment-resistant sepression. Biological Psychiatry (Epub ahead of print).
Sitaram, R., Lee, S., Ruiz, S., Rana, M., Veit, R., & Birbaumer, N. (2011). Real-time
support vector classification and feedback of multiple emotional brain states. Neuroimage, 56(2), 753–765.
�Deep Brain Stimulation for Psychiatric Disorders
15
Warden, D., Rush, A. J., Trivedi, M. H., Fava, M., & Wisniewski, S. R. (2007). The
STAR*D project results: A comprehensive review of findings. Current Psychiatry
Reports, 9(6), 449–459.
Widge, A. S., Dougherty, D. D., & Moritz, C. T. (2014). Affective brain-computer
interfaces as enabling technology for responsive psychiatric stimulation.
Brain-Computer Interfaces, 1(2), 126–136.
Widge, A. S., & Moritz, C. T. (2014). Pre-frontal control of closed-loop limbic neurostimulation by rodents using a brain-computer interface. Journal of Neural Engineering, 11(2), 024001.
ALIK S. WIDGE SHORT BIOGRAPHY
Alik S. Widge is the Director of the Translational NeuroEngineering Laboratory and a clinician in the Division of Neurotherapeutics at Massachusetts
General Hospital. He completed combined MD/PhD training at the University of Pittsburgh and Carnegie Mellon University, followed by psychiatry
residency at the University of Washington. He remains a member of the joint
UW-MIT Center for Sensorimotor Neural Engineering. Dr. Widge’s research
centers around “closed loop” brain stimulators that sense and respond to
ongoing brain activity. He produced the first working demonstration of such
a stimulator in the psychiatric domain, and is now engaged in research to
bring this technology into human use.
http://scholar.harvard.edu/awidge/
AMANDA R. ARULPRAGASAM SHORT BIOGRAPHY
Amanda R. Arulpragasam is a clinical research coordinator within the
Division of Neurotherapeutics at the Massachusetts General Hospital. Her
research focuses on the use of neuroimaging techniques to better understand
psychiatric disorders as well as the mechanism of action of treatment
interventions (such as DBS).
THILO DECKERSBACH SHORT BIOGRAPHY
Thilo Deckersbach, PhD is an Associate Professor of Psychology at Harvard
Medical School. He serves as the Director of Research in the Division of Neurotherapeutics, the Director of Psychology in the Bipolar Clinic and Research
Program and as the Director of the MGH Graduate Student Division at at the
Massachusetts General Hospital in Boston. Dr. Deckersbach’s research has
been supported by the National Institute of Mental Health, NARSAD, TSA,
OCF, and DBDAT. He has published over 95 peer-reviewed papers and book
�16
EMERGING TRENDS IN THE SOCIAL AND BEHAVIORAL SCIENCES
chapters. His functional neuroimaging research (fMRI and PET) focuses on
the interaction of cognitive and emotional processes in bipolar disorder.
DARIN D. DOUGHERTY SHORT BIOGRAPHY
Dr. Darin D. Dougherty is the Director of the Neurotherapeutics Division in
the Department of Psychiatry at MGH, the Director of the Mood Disorders
Section of the Massachusetts General Hospital Psychiatric Neuroimaging
Group, and the Associate Director of the Massachusetts General Hospital
Psychiatric Neuroimaging Group. Dr. Dougherty is also the Director of Medical Education at the Massachusetts General Hospital Obsessive-Compulsive
Disorder Institute and the Co-Director of the Massachusetts General Hospital Trichotillomania Clinic. Additionally, Dr. Dougherty is an Associate
Professor of Psychiatry at Harvard Medical School, a Clinical Associate at
Massachusetts General Hospital and a Visiting Scientist at Massachusetts
Institute of Technology.Dr. Dougherty currently serves on the scientific advisory board for both the Anxiety Disorders Association of America and the
Obsessive Compulsive Foundation. He serves on the Massachusetts General
Hospital Psychiatric Neurosurgery Committee. He also serves on many
editorial boards and award committees. He has given over a hundred invited
lectures and presentations, and is a current member of many professional
societies. In 2003 Dr. Dougherty was awarded a NARSAD Young Investigator Award. In 2005 he was named one of the Future Leaders in Psychiatry.
Dr. Dougherty has co-authored over 100 original articles in peer-reviewed
journals, book chapters, and review articles, and has co-edited two books
on neuroimaging. Currently Dr. Dougherty is the Principal Investigator
or co-Principal Investigator on several government and industry funded
studies investigating neuroimaging and medication and neurosurgery treatments of OCD and mood disorders.Dr. Dougherty received his MD from the
University of Illinois and completed his residency in general psychiatry at
Massachusetts General Hospital. He is a graduate of the Clinical Investigator
Training Program at Harvard Medical School and Massachusetts Institute of
Technology. Dr. Dougherty’s research interests include neuroimaging, neurobiology, psychopharmacology, and neurotherapeutic (device and/or surgical) interventions for the treatment of treatment-refractory psychiatric illness.
RELATED ESSAYS
Positive Emotion Disturbance (Psychology), June Gruber and John Purcell
What Is Neuroticism, and Can We Treat It? (Psychology), Amantia Ametaj
et al.
Peers and Adolescent Risk Taking (Psychology), Jason Chein
�Deep Brain Stimulation for Psychiatric Disorders
17
Delusions (Psychology), Max Coltheart
Misinformation and How to Correct It (Psychology), John Cook et al.
Problems Attract Problems: A Network Perspective on Mental Disorders
(Psychology), Angélique Cramer and Denny Borsboom
Controlling the Influence of Stereotypes on One’s Thoughts (Psychology),
Patrick S. Forscher and Patricia G. Devine
Depression (Psychology), Ian H. Gotlib and Daniella J. Furman
Mental Imagery in Psychological Disorders (Psychology), Emily A. Holmes
et al.
Normal Negative Emotions and Mental Disorders (Sociology), Allan V.
Horwitz
Dissociation and Dissociative Identity Disorder (DID) (Psychology), Rafaële
J. C. Huntjens and Martin J. Dorahy
Computer Technology and Children’s Mental Health (Psychology), Philip C.
Kendall et al.
Cultural Neuroscience: Connecting Culture, Brain, and Genes (Psychology),
Shinobu Kitayama and Sarah Huff
Mechanisms of Fear Reducation (Psychology), Cynthia L. Lancaster and
Marie-H. Monfils
Disorders of Consciousness (Psychology), Martin M. Monti
Cognitive Bias Modification in Mental (Psychology), Meg M. Reuland et al.
Clarifying the Nature and Structure of Personality Disorder (Psychology),
Takakuni Suzuki and Douglas B. Samuel
A Gene-Environment Approach to Understanding Youth Antisocial Behavior (Psychology), Rebecca Waller et al.
Rumination (Psychology), Edward R. Watkins
�