Macroeconomic Effects on Mortality: Issues, Controversies, and Directions for Research
Media
Part of Macroeconomic Effects on Mortality: Issues, Controversies, and Directions for Research
- Title
- Macroeconomic Effects on Mortality: Issues, Controversies, and Directions for Research
- extracted text
-
Macroeconomic Effects on Mortality:
Issues, Controversies, and Directions
for Research
JOSÉ A. TAPIA GRANADOS
Abstract
This essay examines the development of ideas on the macroeconomic effects on mortality. It surveys some nineteenth century views, the early twentieth century contributions of Ogburn and Thomas, the 1970s–1980s debates of Brenner and Eyer, and the
modern views, contributions, and controversies involving Ruhm and other authors
who have tried to demonstrate the empirical support—or the lack of it—for the contentious hypothesis of the procyclical oscillation of mortality. That is the pattern, now
clearly established for many, but unproved for more than a few skeptics, that once
long-term trends are taken away, mortality oscillates with the business cycle, rising
in expansions and declining in recessions. Potential sources of discrepancies, hypothesized or proven mechanisms for procyclical mortality, and related policy issues are
discussed, and the essay concludes by suggesting five questions that future research
should aim to answer.
To the memory of Joe Eyer, 1944–2017
INTRODUCTION
In 2000, Christopher Ruhm’s article “Are recessions good for your health?”
was published in the Quarterly Journal of Economics. Ruhm modeled mortality
rates of the 50 states of the United States, using fixed effects to adjust for time
trends and unobserved variables. He found higher unemployment associated with lower mortality for all causes and for the most important causes of
death; that means that mortality is lower in recessions.1
1. Because space restrictions, only a few selected references are included in the reference list of this
essay. When controversies are cited, only the last article of the debate is referenced as a guide. A fully
referenced version is available from the author on request.
Emerging Trends in the Social and Behavioral Sciences.
Robert Scott and Marlis Buchmann (General Editors) with Stephen Kosslyn (Consulting Editor).
© 2017 John Wiley & Sons, Inc. ISBN 978-1-118-90077-2.
1
2
EMERGING TRENDS IN THE SOCIAL AND BEHAVIORAL SCIENCES
Ruhm’s paper was considered as a path-breaking work in economics.
However, for quite a number of researchers in various fields Ruhm’s results
were puzzling. Epidemiologists and demographers had repeatedly found
that mortality has a gradient by social class and ethnic group, so that those
living on manual work, having lower income, or pertaining to marginalized
groups have higher mortality. Furthermore, unemployed individuals had
been repeatedly found having lower levels of health and higher risk of
death. During recessions, incomes decrease and many become unemployed,
so would it not be logical to expect as a consequence worse health and higher
mortality? When research found the opposite, it generated puzzlement.
ANTECEDENTS OF PUZZLEMENT
In the first half of the nineteenth century, the ideas on population of Thomas
Robert Malthus raised major controversies. Malthus attacked the views on
social progress of William Godwin and the Marquis de Condorcet, who
in today’s parlance would be left-wing radicals. For Malthus, unavoidable scarcity due to population increasing faster that food would lead to
repeated “checks” in which outbreaks of famine, epidemics, and war would
reestablish the equilibrium between human numbers and food availability.
In 1845, one of Malthus’s critics, Friedrich Engels, claimed that it was not
overpopulation but recurrent commercial crises that brought misery and
were often linked to epidemics and general malaise. Twenty years later,
Engels’s friend and protégée Karl Marx reported in Das Kapital a quite
different thing. Marx said, citing reports of medical inspectors, that health
had improved among the workers in the English textile districts during
the crisis of the 1860s, when cotton supplies had ceased arriving England
because the U.S. Civil War. Many had become unemployed but, in general,
health had improved during the crisis, as workers had ceased being exposed
to the insalubrious environment of the factories, and mothers had now
time to breastfeed their children and no money to buy them Geoffrey’s
Cordial—an opiate mixture which in those times was often administered to
babies to keep them quiet.
It was, however, the notion of a link between economic crises, overpopulation, and excess mortality that took hold. Thus in 1898, in a study on commercial crises in England, Mijail Tugan-Baranovski concluded after a very superficial examination of the data that crises were associated with increased mortality. A much more careful study authored by William Ogburn and Dorothy
Thomas three decades later, in 1922, showed exactly the opposite, a positive
correlation of detrended annual series of business indicators and the mortality rate, which proved that economic depressions were associated with lower
mortality. Ogburn and Thomas were puzzled by this finding, but after much
Macroeconomic Effects on Mortality: Issues, Controversies, and Directions for Research
3
consideration and further study they thought it was real, as they found it
both in U.S. and British data.
MORTALITY AND THE BUSINESS CYCLE
The oscillations of economic activity between boom and bust, prosperity
and depression, or expansion and recession have been called business
cycles, trade cycles, industrial cycles, and crisis cycles, but such abundance
of terminology goes along with the inability of the economic profession
to agree on the causes of the phenomenon. In the 1860s, Clément Juglar
in Les Crises commerciales et leur retour periodique en France, en Angleterre,
et aux Etats-Unis and Karl Marx in Das Kapital theorized on the cause
of crises. Both attributed crises to the inner workings of the free-market
system, but their contributions had little resonance among economists who
were paying more attention to outstanding members of the profession
like W. S. Jevons and H. L. Moore, who attributed crises to influences of
the Sun or the planet Venus. It took a while for these astral theories to go
away, despite that they were clearly at odds with the facts. In 1920, an
economist-geographer, Ellsworth Huntington, proposed that recessions are
due to unidentified biological factors that generate peaks in mortality and
impact on the spending and investing psychology of the public. Huntington
was noticing the same correlation between death rates and macroeconomic
conditions that Ogburn and Thomas would notice later, but he was looking for causality in the opposite direction, that is, from mortality to the
economy.
In the 1930s, the world sank in depression and joblessness increased rapidly.
In Cycles and crisis, published in 1936, the German economist Wilhelm Roepke
wrote that the general contraction of economic activity of the depression was
associated with dismissed workmen, closed workshops, rusting machines,
and the human tragedies bound up with them, including a rise in death
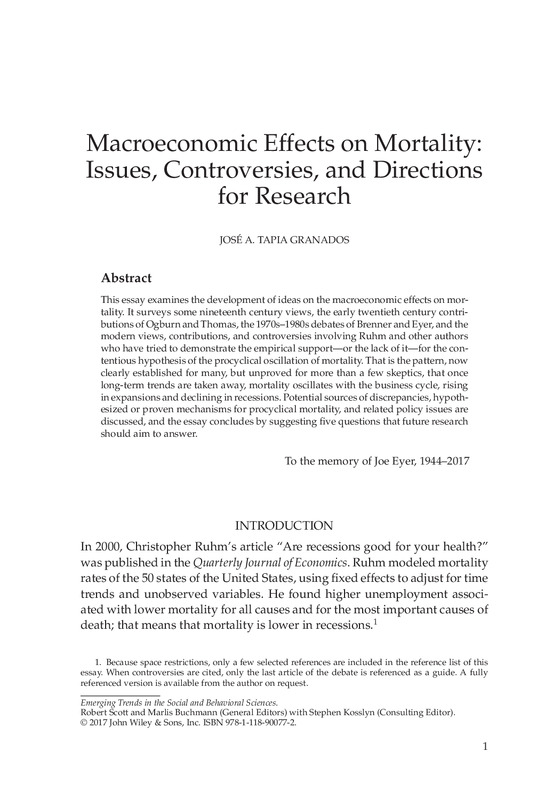
rates. But, alas, he was totally wrong about this, as actually mortality had
decreased, puzzling public health workers (Tapia Granados & Diez Roux,
2009). It had been in the expansionary twenties that mortality had stagnated
or increased (Figure 1). However, at the time all this was barely registered.
After the depression and the war passed, new data now available made
obvious that mortality was secularly declining in many countries. In 1958, a
leading demographer and economist, George Stolnitz, claimed that disease
control, that is, advances in medicine and health care, had been the most
influential factor for mortality reduction. This was the typical view in the
1950s and 1960s, though the long-term decline in mortality was also thought
to be influenced by economic growth. Interestingly, in the United States, the
1950s and 1960s were economically prosperous but mortality declined at
4
EMERGING TRENDS IN THE SOCIAL AND BEHAVIORAL SCIENCES
22
20
18
16
14
12
10
8
6
Nonwhite
White
1920
1930
1940
1950
1960
1970
Figure 1 Age-adjusted mortality (per 100,000 population) for whites and
nonwhites in the U.S. civilian population, 1920–1970. Source: Historical Statistics
of the United States.
a much lower rate than in the 1930s and 1940s (Figure 1). The short-term
negative association between economic growth and mortality that Ogburn
and Thomas had discovered in the 1920s had been totally forgotten.
It was rediscovered in 1977 by a biologist at the University of Pennsylvania, Joe Eyer. By inspecting U.S. graphs of mortality and unemployment for
1870–1975, Eyer noticed that they evolved mirroring each other, so that peaks
in one series coincided with troughs in the other.
Eyer knew the 1920s publications by Dorothy Thomas and proposed several hypotheses to explain what he called the Thomas effect, that is, the rise
of mortality during economic expansions. He attributed it to higher levels of
stress at work, increasing overtime, overwork, and migration, and the subsequent decline in networks of social support and increase in the consumption
of harmful substances.
It was also during the 1970s that Thomas McKeown, a British historian
of medicine, published a series of analyses of population data. McKeown’s
basic conclusion was that population growth since the late eighteenth
century was mostly due to a drop in death rates caused by rising standards
of living. The basic mechanism would be a higher level of resistance to
infection due to an improvement in nutrition. For McKeown, better hygiene,
public health measures, and improved medicine had had only a limited
role in the historical decline of mortality. Though McKeown’s contributions
referred to long-term processes, and to the already gone time when most
deaths were due to infectious disease, they probably created a fertile ground
for the ideas of Harvey Brenner.
Brenner’s basic claim was that recessions raise mortality rates, though
the effect occurs, he said, with a lag. Brenner was very unclear about this
lag, stating in some papers it is just a few years, in others that it is 10
years, or even more. Given that recessions recur at variable periods—few
years or sometimes even more than a decade—this lagged effect cannot
Macroeconomic Effects on Mortality: Issues, Controversies, and Directions for Research
5
explain that troughs of mortality coincide with recessions, that is, with
peaks of unemployment. Brenner used econometric methods very obscurely
explained, and probably many readers, including reviewers, did not understand them. There were, however, researchers, starting with Eyer, who did
not buy Brenner’s main idea, that is, his “demonstration” of recessions
raising mortality with a lag. Brenner’s work was criticized as confusing and
irreproducible, but Brenner never answered his critics. All this was later
summarized as leading to considerable skepticism about Brenner’s data and
conclusions (Kasl & Jones, 2000).
PROCYCLICAL MORTALITY AS A CONTENTIOUS HYPOTHESIS
Since 2000, when Ruhm’s paper appeared, researchers from various fields of
social science have found in different countries and periods that over and
above long-term trends, mortality oscillates procyclically, that is, increasing
during expansions and decreasing during recessions—more than 30 of these
publications are cited elsewhere (Tapia Granados & Ionides, 2017). However,
incredulity persists among researchers who are reluctant to believe that recessions with the associated joblessness and loss of income are not harmful for
health and survival.
One of these investigators, Ralph Catalano, tested in a 1998 study the effect
of macroeconomic changes on mortality. As a kind of control, Catalano
included Danish data as a covariate in his models for the United States, an
unconventional method that no one has tried later. Catalano concluded that
mortality declined in years following increases in per capita national income
above long-term trend, that is, that expansions reduce mortality with a lag.
This is Brenner’s thesis with other words. However, Catalano seems to have
changed his views, as in recent controversies on the mortality effects of
the Great Depression (Bruckner, Noymer, & Catalano, 2013) and the Great
Recession (Tapia Granados & Ionides, 2016) he defended the view that
neither of them had any significant positive or negative effect on mortality.
In passing, it has to be said that maintaining that recession has no effect on
mortality while expansion stimulates its decline would not be admissible on
logical grounds.
In another controversy on the Great Depression, David Stuckler, Sanjai
Basu, and others argued that the only mortality effect of it was, as that
of other recessions, to raise suicides and reduce traffic fatalities, without
any detectable effect on major causes of death (Tapia Granados, 2013a).
These researchers reached this conclusion from investigating 1970–2007
data from 26 EU countries. This was a study that unfortunately conflated
data from two very different scenarios: the sustained decline of mortality rates—which indeed accelerated slightly during recessions—during
6
EMERGING TRENDS IN THE SOCIAL AND BEHAVIORAL SCIENCES
the 1980s and 1990s in Western Europe, and the demographic disaster
in Eastern Europe during the 1990s, when major increases in mortality occurred during the crisis transition to a market economy. Because
of the heterogeneity of the data, the study conclusions are hopelessly
unreliable.
It were also Stuckler and Basu, who in a book melodramatically entitled The
Body Economic—Why Austerity Kills, argued that during economic crises government policies determine whether mortality will increase or decline. Such
an optimistic view on the ability of government policy to modify quickly a
demographic variable as complex as mortality was a flawed diagnosis (Tapia
Granados, 2013b). It was demonstrated so by the fact that since 2008 mortality has significantly declined in Europe, particularly in Greece and Spain
where both the severity of the recession and the application of austerity policies have been outstanding (Regidor et al., 2016; Tapia Granados & Ionides,
2017; Tapia Granados & Rodriguez, 2015).
Further controversies on similar issues have occurred (Tapia Granados,
2014), and everything suggests that they will continue, as the sources of these
debates are well-rooted ideas. Doubtlessly, different investigators would
give different answers to the question of what specific misunderstandings
or erroneous ideas underlie these arguments. From the point of view of the
present writer, who is an interested party, two deep-rooted beliefs are the
basis of the visceral rejection of the hypothesis of procyclical mortality by
quite a number of investigators: first is the belief that a growing market
economy is good for everyone, something that economists have preached
since Adam Smith; second is the view that the level of income is the major
determinant of the probability of death, something that can be erroneously
inferred from modern public health research, which rather has shown that
working and living conditions and the social context—including what
epidemiologists call “social support,” —are key determinants of the risk of
death.
Looking at more superficial reasons for discrepancies, it is obvious that
sometimes they refer to misunderstandings on the analysis of time series
(Tapia Granados & Ionides, 2016), the nature of the business cycle, or the relation between causal structures and regression analysis. Thus in an investigation testing whether economic fluctuations have an impact on mortality, such
variables as traffic volume and tobacco consumption were included in a multivariate regression with the death rate as dependent variable (Economou,
Nikolaou, & Theodossiou, 2008). Since expansions can be harmful precisely
because they involve increased traffic and tobacco consumption, this is a perfect recipe for obtaining spurious results.
Complicating research on these issues and fueling skepticism is the fact that
methods to ascertain causal links between time-series variables have often
Macroeconomic Effects on Mortality: Issues, Controversies, and Directions for Research
7
raised controversy in social sciences, particularly in macroeconomics, where
major disagreements exist.
In early investigations of macroeconomic effects on health, the unit of
analysis was usually a whole nation, with the analysis reduced to a bivariate
analysis of time-series data. But most time series of economic indicators
and health variables are annual, and this usually means series that rarely go
beyond a hundred observations, and usually much shorter. Panel analyses
with disaggregated data for smaller geographical units have greater statistical power, but they raise two issues: what is the proper level of aggregation
(Lindo, 2015) and the violation of the assumptions of linear regression which
is caused by the use of linear trends and can bias the results (Ionides, Wang,
& Tapia Granados, 2013).
In 2015, Ruhm analyzed U.S. national-, state-, and county-level data
1976–2013 to investigate whether economic crises affect mortality “in the
same way as less severe downturns.” He concluded that the answer is yes,
so that both recessions and crises reduce death rates, with crises having an
effect on mortality that is about twice as strong as what would be expected
due to the elevated unemployment rates alone. In the operational definition
of economic crisis of this study, a crisis is just a severe recession as indexed
by unemployment reaching more or less arbitrarily determined “high
levels.” Ruhm admitted that this definition is arguable. For Wesley Mitchell,
the pioneer in business-cycle research, in the context of market economies,
“crisis,” “depression,” and “recession” are terms that refer basically to the
same phenomenon; they only suggest different intensities of it. On the other
hand, the famines that occurred in the USSR in 1932–1933, or in the Netherlands or India during World War II, or the extreme economic disruption that
occurred in Eastern Europe in the 1990s are also “economic crises,” in all
of which there were substantial increases in mortality. However, these are
economic crises of a very different nature to the recessions or depressions
of, say, the early 1980s or the last years of the past decade, which appeared
under “normal” social life in settled market economies. In all these cases,
mortality continued its secular decline, and dropped even faster.
A new example of the proneness of quite a number of researchers to
look for reasons to deny the procyclical oscillation of mortality is a recent
paper by Arthi et al. (2017) who propose a “migration bias” as the cause of
the “observed” procyclical oscillation of mortality. This oscillation would
actually be a statistical artifact. According to Arthi et al. (2017) selective
migration—toward booming regions and away from depressed areas—bias
the denominator of mortality rates causing mortality to seemingly oscillate
procyclically, when in reality it does not oscillates, or even oscillates countercyclically. The reasoning of the paper is tortuous, and its results are at
odds with many studies showing a procyclical oscillation of mortality using
8
EMERGING TRENDS IN THE SOCIAL AND BEHAVIORAL SCIENCES
national data (for instance in the USA, UK, Sweden, and Japan). But for sure
it will find a receptive audience.
POLICY ISSUES
Leading economists like Paul Samuelson, Milton Friedman, or Robert
Lucas claimed at different times the ability of economic policy guided by
macroeconomic principles to prevent major oscillations of economic activity.
However, the interventionist or laissez faire policies these authors advocated
were remarkably different. Indeed, the major economic downturns observed
around the turn of the century in most of the developing world and in
2008 in the global economy suggest that governments are rather unable to
prevent them. Furthermore, economists are seriously divided on what is to
be done to prevent or ameliorate recessions.
In spite of all that, some health researchers are convinced that it is government policy that determines whether an economic crisis will have or not
harmful effects on mortality. The idea is far from being demonstrated; indeed,
as has been argued here, the weight of evidence favors the view that mortality
oscillates procyclically, so that recessions stimulate the decline of mortality
independently of government policy.
Ruhm, who is arguably the contemporary researcher who has contributed
more to the view that expansions have harmful effects on mortality, has
claimed that contractionary macroeconomic policies are not justified, as
recessions “have overwhelmingly negative consequences, even if they
do not harm physical health.” Obviously, the negative consequences
meant by Ruhm are the business failures and the destruction of jobs
that characterize recessions and trigger social distress. But what about
policies intended to prevent the harmful effects of expansion? Ruhm
has suggested establishing economic incentives to reduce unhealthy
behaviors, and to promote healthier conditions of work—with reductions in overtime and mandatory expansion of vacation time. Policies
to reduce unhealthy consumption have been indeed implemented in
some countries, though almost exclusively for alcohol and tobacco products. Interestingly, in the field of public health, similar policies applied
to the consumption of fossil fuel have been recommended not only to
prevent climate change but also as potentially having major effects in
reducing traffic mortality, cardiovascular and respiratory diseases, and
many other causes of death. However, as illustrated by recent political
developments on climate change, in the short run the implementation
of such policies is very unlikely in any country, as they encroach on
business profits and therefore are strongly opposed by the business
community.
Macroeconomic Effects on Mortality: Issues, Controversies, and Directions for Research
9
Given disagreements inside economics on the effect of policies, the not
uncommon skepticism on the procyclical oscillation of mortality among
health researchers, as well as the scarce political feasibility of specific
policies to dampen the oscillation of mortality during expansions, to reach
any consensus to recommend this kind of policies seems very unlikely in the
near future. Thus, trying to develop theoretical foundations for such policies
does not look at all a fertile ground for work.
FIVE QUESTIONS THAT FUTURE RESEARCH SHOULD AIM
TO ANSWER
The starting point here is considering the procyclical oscillation of mortality
as a hypothesis supported by substantial evidence. For researchers who are
skeptical about it, what follows will probably make little sense.
1. What is the Connection Between the Epidemics of Prescription Drug
Poisoning, Other Iatrogenic Deaths, and the Business Cycle?
In the United States, the highly publicized epidemic of fatalities caused by
poisoning with prescription drugs seems to have grown with the recession,
that is, countercyclically (Ruhm, 2015). This epidemic of deaths caused
by prescribed medicines has obviously links with the larger chapter of
medical errors, estimated as the third leading cause of death in the United
States (Makary & Daniel, 2016). Now, all this raises the issue whether
business-cycle-related changes in the level of access or intensity of medical
care might be connected with procyclical mortality. According to reports of
the Centers for Disease Control (CDC), the overall U.S. death rate increased
in 2015 for the first time in a decade, exactly at the same time that Obamacare
was expanding access to health services. This is of course only one data
point, but it raises major questions.
2. Is Mortality Becoming Less Procyclical?
The procyclical oscillation of mortality might be disappearing because
dampening by the increasing weight in mortality of fatalities which are
either countercyclical (e.g., analgesic overdoses) or acyclical (cancer). Versus
this view, recent studies rather suggest the opposite. Lindo, in a study with
U.S. county data which provides important methodological insights has
found an intense procyclical oscillation of mortality and has rejected the
view that mortality would be becoming less procyclical (Lindo, 2015). Furthermore, in a number of studies, increased unemployment rates in recent
times (e.g., in U.S. states or EU nations) have been found associated with
10
EMERGING TRENDS IN THE SOCIAL AND BEHAVIORAL SCIENCES
large drops in mortality, which reinforce the hypothesis of procyclicality
of the death rate. At any rate, studies formally testing the hypotheses of
procyclical mortality and its potential dampening in recent times would
contribute to improve our understanding of these issues. China and India
are two countries in which testing these hypothesis would be particularly
valuable.
3. What are the Major Mechanisms for Procyclical Mortality?
Advances in understanding the mechanisms for procyclical mortality have
occurred. From an analysis of U.S. data, it has been concluded that about
a third of procyclical mortality is attributable to variations in atmospheric
pollution (Heutel & Ruhm, 2013). On the other hand, evidence that procyclical mortality due to injuries is connected with the procyclical oscillation of
industrial and recreational traffic as well as workplace activity and hiring
has continued piling up (Asfaw, Pana-Cryan, & Rosa, 2011; French & Gumus,
2014). Proposed connections between procyclical mortality and changes in
staffing of institutions for the elderly were suggested, but have been seen
with skepticism. A study using European data showed shorter working
hours associated with higher mortality (Johansson, 2004), a result that seems
to contradict the old idea that lower mortality in recessions may be linked to
the procyclical character of working time, overtime, and work-related stress.
However, this was just an isolated study, and indeed institutional factors
may modify the business-cycle character of hours worked, which may
measure different things in different countries. At any rate, the potential
relation of work hours, overtime, stress levels in the working environment,
and connected issues with the oscillation of mortality seems a largely
unexplored field worthy of investigation.
A still unpublished study has investigated the association of economic conditions in the area of residence with the level of risk factors for cardiovascular
disease in a sample of residents, finding that systolic and diastolic blood
pressure rise and physical activity drops during expansions. These can be
important findings opening major avenues for future research.
4. Who is Hurt, Who Benefits from Procyclical Mortality?
A recent study demonstrated that mortality decline significantly accelerated
in Spain during the recession that started in 2008 (Regidor et al., 2016). Mortality was found to be the highest in the group of low socioeconomic status
(SES) and the lowest in the group of high SES. The annual reduction in mortality during the recession years 2008–2011 was almost without exception
in each SES group greater than the reduction in 2004–2007, that is, during
Macroeconomic Effects on Mortality: Issues, Controversies, and Directions for Research
11
the previous expansion. Furthermore, the acceleration of mortality decline
during the recession was intense in the group of low SES, but very small in
the group of high SES. The conclusion was that mortality decline accelerated
during the recession, particularly in the group of low SES and, likely as a consequence of drops in the exposure to risk factors, probably more important
for individuals of low SES.
It seems that groups of lower SES benefit the most from the acceleration
of mortality decline during recessions. In the United States during the early
1930s, mortality dropped in whites and nonwhites and males and females,
but it dropped the most in African-American men (Tapia Granados & Diez
Roux, 2009). The mortality gap between whites and nonwhites had clearly
widened in the “roaring” 1920s, then narrowed in the depressed 1930s
(Figure 1). In Finland, in the severe recession of the early 1990s, mortality
declined the most among households obtaining income from manual
occupations (Tapia Granados, 2007). In Japan, stagnation during the 1990s
was associated with dramatic changes in occupational patterns of mortality,
as the health of managers and professionals deteriorated while that of sales
staff and blue collar workers did not, all of which led to a major reduction
or even reversal of the usual patterns of health inequality (Wada et al.,
2012). In all these studies, low SES groups benefit more from the reduction
in mortality during recessions, so that health inequality tend to diminish.
If that is the case, not only mortality but mortality inequalities would be
procyclical. A study with U.S. data (Edwards, 2008) seems at present the
only investigation perhaps inconsistent with the hypothesis that mortality
inequalities by SES are procyclical.
5. Is Economic Growth Presently Hindering Health Progress?
This is probably the most important question connected with the hypothesis
of procyclical mortality. It is a key question because economic growth as a
panacea for all social ills is an entrenched idea in our culture. So much so that
that two authors, Suchit Arora and R. F. Swift, “demonstrated” in the past the
cointegration between the level of health, as measured by life expectancy at
birth (LEB), and the level of income, as measured by GDP per capita. This
cointegration was also one of the “contributions” of Harvey Brenner.
Cointegration between LEB and income per capita means that in the long
run each variable will follow the path of the other, so that higher levels of
health will be obtained by raising levels of income. Versus that idea, supposedly proved by tortuous econometrics by Arora and Swift, what recent studies on the long-term evolution of mortality have shown is that, if there was
a positive link between economic growth and population health, that link
has disappeared in recent decades (Cutler, Deaton, & Lleras-Muney, 2006;
12
EMERGING TRENDS IN THE SOCIAL AND BEHAVIORAL SCIENCES
Preston, 2007). This is an idea that still provokes the suspicion and rejection
of those who more or less enthusiastically defend the thesis of “wealthier is
healthier” (Mackenbach, 2007).
The hypothesis of procyclical mortality is also counterintuitive because it
suggests that economic growth is harmful for health, while economic stagnation or contraction is beneficial. Thus an epidemiologist mocked once the
hypothesis of procyclical mortality by asking whether public health people
should advocate recessions. But, should they?
Let start from assuming that we agree that mortality is procyclical, so that
it deviates from a long-term declining trend upward in the expansions and
downward in the recessions. Now, this oscillation can be considered as having no net effect on the long-term evolution of mortality, as the excess mortality during the expansion may be compensated by lower mortality during
the recession. Then, in the long run, wider or flatter macroeconomic oscillations would make no difference in the evolution of mortality. But in most
business cycles, the expansion is longer than the recession, and therefore the
above-trend mortality of the expansion would not be compensated by the
below-trend mortality during the recession. If that is the case, longer or faster
expansions would mean a longer accumulation of over-trend mortality; that
is, faster or more maintained GDP growth would cause slowly increasing or
even decreasing LEB, while longer or deeper recessions would mean longer
accumulation of below-trend mortality, that is, faster increase of LEB. Quite
substantial evidence seems to support this hypothesis.
With one of the oldest and best demographic statistics of the world,
Sweden has been the object of many demographic studies and controversies.
Using Swedish data, Edward Ionides and I showed in 2008 that in the past
two centuries there was a reversal of the relation between economic growth
and health progress. Throughout the nineteenth century GDP growth was
positively associated with the annual decline in mortality, or the gain in
LEB, but the relation became weaker as time passed and was completely
reversed in the second half of the twentieth century, when economic growth
appears inversely associated with health progress, with higher annual GDP
growth implying lower annual reductions in mortality, or gains in LEB.
This paper, like those by Arora and Swift, have been basically unnoticed
by health researchers. Unfortunately, published research is often ignored
rather than replicated or refuted, which does not contribute to scientific
progress.
While the hypothesis that economic growth has become a hinder for health
progress is clearly supported by the case of Sweden, additional “circumstantial evidence” is abundant from other countries and periods. Thus in
the UK, Amartya Sen showed an inverse relation between the decennial
rate of GDP growth in the period 1900–1960 and the decennial increase of
Macroeconomic Effects on Mortality: Issues, Controversies, and Directions for Research
13
LEB in England and Wales (Sen, 2001), a finding that was later replicated
for a larger timeframe of almost two centuries. In the United States, the
decades prior to the Civil War of the 1860s saw rapid economic growth at the
same time that the stature of native-born white males dropped, revealing
a deterioration of population health (Haines, Craig, & Weiss, 2003). Then,
in the twentieth century, during the “roaring” 1920s, mortality stagnated or
increased, while in the depressed 1930s it quickly dropped, and during the
“prosperous” 1950s and 1960s it basically stagnated (Figure 1). In the two
most populous nations of the world, China and India, the past half century
saw quick mortality decline in the decades of economic stagnation and slow
mortality decline when economic growth accelerated (Cutler et al., 2006).
The relation seems to be observed also in African countries, where high GDP
growth has been associated with poor improvements in infant mortality and
other health indicators in recent decades. Thus Botswana and South Africa
had much higher GDP growth and much smaller reductions in mortality
than Morocco and Ethiopia.
According to World Bank data, in 2014 Japan was the nation with the
highest LEB (83.6 years), followed by Spain, with the highest LEB in Europe
(83.1 years). Now, the remarkable thing is that these two countries have had
a very poor economic performance in recent decades, with Japan basically in
chronic stagnation since the 1990s and Spain suffering the worst recessions
and the highest levels of unemployment in Europe since the early 1980s. The
recent Great Recession has been associated with major gains in LEB in Spain,
Greece, and the Baltic States, that is, the economies where the recession was
the most severe. Contrarily, among the high-income countries of the OECD,
the United States and Denmark have been often considered as perhaps
the most efficient economies in term of flexible and well-performing labor
markets which allow more sustained GDP growth and less unemployment.
At the same time, though, both countries are the OECD laggards in terms of
population health.
The common view that business prosperity and GDP growth are what we
need to solve social problems seems at odds with the aforementioned facts,
but it is also questioned by something more important, the fact that faster
GDP growth means both at the level of national economies and the global
economy, greater emissions of CO2 (Tapia Granados, Ionides, & Carpintero,
2012) and thus a faster approximation toward what could be the worst
human-made catastrophe in history. Of course, advocates of zero growth
usually ignore the obvious fact that in our economic system no growth
represents rising unemployment rates and social malaise. But those who are
enthusiastic about economic growth are very often oblivious to the harmful
consequences of it.
14
EMERGING TRENDS IN THE SOCIAL AND BEHAVIORAL SCIENCES
The function of social science, Joan Robinson once said, “is quite different
from that of the natural sciences—it is to provide society with an organ of
self-consciousness.” Let us hope that humanity may generate a sufficient
level of self-consciousness before it goes down into a man-made black hole.
Perhaps research on the macroeconomic effects on health can contribute
something to that endeavor.
REFERENCES
Arthi, V., Beach, B., & Hanlon, W. (2017). Estimating the recession-mortality relationship when migration matters. NBER Working Paper 23507.
Asfaw, A., Pana-Cryan, R., & Rosa, R. (2011). The business cycle and the incidence of
workplace injuries: Evidence from the U.S.A. Journal of Safety Research, 42(1), 1–8.
Bruckner, T. A., Noymer, A., & Catalano, R. A. (2013). Life expectancy during
the Great Depression in eleven European countries. Population and Development
Review, 39(1), 57–74.
Cutler, D., Deaton, A. S., & Lleras-Muney, A. (2006). The determinants of mortality.
Journal of Economic Perspectives, 20, 97–120.
Economou, A., Nikolaou, A., & Theodossiou, I. (2008). Are recessions harmful to
health after all?: Evidence from the European Union. Journal of Economic Studies,
35(5), 368–384.
Edwards, R. D. (2008). Who is hurt by procyclical mortality? Social Science & Medicine,
67(12), 2051–2058.
French, M. T., & Gumus, G. (2014). Macroeconomic fluctuations and motorcycle fatalities in the U.S. Social Science & Medicine, 104, 187–193.
Haines, M. R., Craig, L. A., & Weiss, T. (2003). The short and the dead: Nutrition,
mortality, and the "antebellum puzzle" in the United States. Journal of Economic
History, 63(2), 382–413.
Heutel, G., & Ruhm, C.J. (2013). Air pollution and procyclical mortality. NBER Working
Paper. 2013(18958).
Ionides, E., Wang, Z., & Tapia Granados, J. A. (2013). Macroeconomic effects on mortality revealed by panel analysis with nonlinear trends. Annals of Applied Statistics,
7(3), 1362–1385.
Johansson, E. (2004). A note on the impact of hours worked on mortality in the OECD.
European Journal of Health Economics, 4, 335–340.
Kasl, S. V., & Jones, B. A. (2000). The impact of job loss and retirement on health. In L.
F. Berkman & I. Kawachi (Eds.), Social epidemiology (pp. 118–136). New York, NY:
Oxford University Press.
Lindo, J. M. (2015). Aggregation and the estimated effects of economic conditions on
health. Journal of Health Economics, 40, 83–96.
Mackenbach, J. P. (2007). Did Preston underestimate the effect of economic development on mortality? International Journal of Epidemiology, 36(3), 496, 497; 502–503.
Makary, M. A., & Daniel, M. (2016). Medical error—the third leading cause of death
in the US. BMJ, 353.
Macroeconomic Effects on Mortality: Issues, Controversies, and Directions for Research
15
Preston, S. H. (2007). On ’The changing relation between mortality and level of economic development’. International Journal of Epidemiology, 36(3), 502–503.
Regidor, E., Vallejo, F., Tapia Granados, J. A., Viciana-Fernández, F. J., de la Fuente, L.,
& Barrio, G. (2016). Faster mortality decline in low socioeconomic groups during
the economic crisis: Authors’s reply. Lancet, 389, 1794–1795.
Ruhm, C.J. (2015). Health effects of economic crises. NBER Working Paper 21604.
Sen, A. (2001). Economic progress and health. In D. Leon & G. Walt (Eds.), Poverty,
inequality, and health: An international perspective (pp. 333–345). Oxford, England:
Oxford University Press.
Tapia Granados, J. A. (2007). Case Study A2: Do health inequalities increase when
employment grows? In J. Benach, C. Muntaner & V. Santana (Eds.), Employment
conditions and health inequalities - Final report to the WHO Commission on Social Determinants of Health (CSDH) prepared by the Employment Conditions Knowledge Network
(EMCONET). Geneve, Switzerland: WHO.
Tapia Granados, J. A. (2013a). Health and the Great Depression: A reply to Stuckler
et al. Journal of Epidemiology and Community Health, 67(12), 1073–1074.
Tapia Granados, J. A. (2013b). A flawed diagnosis: Book review of The Body Economic:
Why Austerity Kills. Science, 341, 1176–1177.
Tapia Granados, J. A. (2014). The Great Recession, a cause of health improvement?
Salud Colectiva (Buenos Aires), 10(1), 101–108.
Tapia Granados, J. A., & Diez Roux, A. V. (2009). Life and death during the Great
Depression. Proceedings of the National Academy of Sciences of the United States of
America, 106, 17290–17295.
Tapia Granados, J. A., & Ionides, E. L. (2016). Statistical evidence shows that mortality
tends to fall during recessions: A rebuttal to Catalano and Bruckner. International
Journal of Epidemiology, 45(5), 1683–1685.
Tapia Granados, J. A., & Ionides, E. L. (2017). Population health and the economy:
Mortality and the Great Recession in Europe. Health Economics.
Tapia Granados, J. A., Ionides, E. L., & Carpintero, O. (2012). Climate change and
the world economy: Short-run determinants of atmospheric CO2 . Environmental
Science & Policy, 21, 50–62.
Tapia Granados, J. A., & Rodriguez, J. M. (2015). Health, economic crisis, and austerity: A comparison of Greece, Finland and Iceland. Health Policy, 119(7), 941–953.
Wada, K., Kondo, N., Gilmour, S., Ichida, Y., Fujino, Y., Satoh, T., & Shibuya, K. (2012).
Trends in cause specific mortality across occupations in Japanese men of working
age during period of economic stagnation, 1980–2005. BMJ, 344, e1191.
JOSÉ TAPIA GRANADOS SHORT BIOGRAPHY
José A. Tapia Granados joined Drexel University after spending 11 years
as a Researcher and Lecturer at the University of Michigan in Ann Arbor.
Prior to that, he lived and worked in New York City, Baltimore, Washington, D.C., and Madrid, Spain, where he practiced medicine briefly as a primary care doctor. Working at the World Health Organization headquarters
16
EMERGING TRENDS IN THE SOCIAL AND BEHAVIORAL SCIENCES
in Washington, D.C. brought him to the United States in 1989. His research
and teaching focus on the intersection of public health, economic issues, and
social science.
RELATED ESSAYS
The Great Recession and Young Adults’ Labor Market Outcomes around the
World (Sociology),Arnaldo Mont’Alvao and Monica K. Johnson
Inefficiencies in Health Care Provision (Economics), James F. Burgess et al.
Labor Market Instability, Labor Market Entry, and Early Career Development (Sociology), Michael Gebel
The Reorganization of Work (Sociology), Charles Heckscher
Family Formation in Times of Labor Market Insecurities (Sociology), Johannes
Huinink
Social Network Analysis in the Study of Ethnic Inequalities (Psychology),
Frank Kalter
Social, Psychological, and Physiological Reactions to Stress (Psychology),
Bruce S. McEwen and Craig A. McEwen
Health and Social Inequality (Sociology), Bernice A. Pescosolido
Limits to Human Longevity (Sociology), Samuel H. Preston and Hiram
Beltrán-Sánchez
Social Relationships and Health in Older Adulthood (Psychology), Theodore
F. Robles and Josephine A. Menkin
The Role of Cultural, Social, and Psychological Factors in Disease and Illness
(Sociology), Robert A. Scott
Incarceration and Health (Sociology), Christopher Wildeman
-
Macroeconomic Effects on Mortality:
Issues, Controversies, and Directions
for Research
JOSÉ A. TAPIA GRANADOS
Abstract
This essay examines the development of ideas on the macroeconomic effects on mortality. It surveys some nineteenth century views, the early twentieth century contributions of Ogburn and Thomas, the 1970s–1980s debates of Brenner and Eyer, and the
modern views, contributions, and controversies involving Ruhm and other authors
who have tried to demonstrate the empirical support—or the lack of it—for the contentious hypothesis of the procyclical oscillation of mortality. That is the pattern, now
clearly established for many, but unproved for more than a few skeptics, that once
long-term trends are taken away, mortality oscillates with the business cycle, rising
in expansions and declining in recessions. Potential sources of discrepancies, hypothesized or proven mechanisms for procyclical mortality, and related policy issues are
discussed, and the essay concludes by suggesting five questions that future research
should aim to answer.
To the memory of Joe Eyer, 1944–2017
INTRODUCTION
In 2000, Christopher Ruhm’s article “Are recessions good for your health?”
was published in the Quarterly Journal of Economics. Ruhm modeled mortality
rates of the 50 states of the United States, using fixed effects to adjust for time
trends and unobserved variables. He found higher unemployment associated with lower mortality for all causes and for the most important causes of
death; that means that mortality is lower in recessions.1
1. Because space restrictions, only a few selected references are included in the reference list of this
essay. When controversies are cited, only the last article of the debate is referenced as a guide. A fully
referenced version is available from the author on request.
Emerging Trends in the Social and Behavioral Sciences.
Robert Scott and Marlis Buchmann (General Editors) with Stephen Kosslyn (Consulting Editor).
© 2017 John Wiley & Sons, Inc. ISBN 978-1-118-90077-2.
1
2
EMERGING TRENDS IN THE SOCIAL AND BEHAVIORAL SCIENCES
Ruhm’s paper was considered as a path-breaking work in economics.
However, for quite a number of researchers in various fields Ruhm’s results
were puzzling. Epidemiologists and demographers had repeatedly found
that mortality has a gradient by social class and ethnic group, so that those
living on manual work, having lower income, or pertaining to marginalized
groups have higher mortality. Furthermore, unemployed individuals had
been repeatedly found having lower levels of health and higher risk of
death. During recessions, incomes decrease and many become unemployed,
so would it not be logical to expect as a consequence worse health and higher
mortality? When research found the opposite, it generated puzzlement.
ANTECEDENTS OF PUZZLEMENT
In the first half of the nineteenth century, the ideas on population of Thomas
Robert Malthus raised major controversies. Malthus attacked the views on
social progress of William Godwin and the Marquis de Condorcet, who
in today’s parlance would be left-wing radicals. For Malthus, unavoidable scarcity due to population increasing faster that food would lead to
repeated “checks” in which outbreaks of famine, epidemics, and war would
reestablish the equilibrium between human numbers and food availability.
In 1845, one of Malthus’s critics, Friedrich Engels, claimed that it was not
overpopulation but recurrent commercial crises that brought misery and
were often linked to epidemics and general malaise. Twenty years later,
Engels’s friend and protégée Karl Marx reported in Das Kapital a quite
different thing. Marx said, citing reports of medical inspectors, that health
had improved among the workers in the English textile districts during
the crisis of the 1860s, when cotton supplies had ceased arriving England
because the U.S. Civil War. Many had become unemployed but, in general,
health had improved during the crisis, as workers had ceased being exposed
to the insalubrious environment of the factories, and mothers had now
time to breastfeed their children and no money to buy them Geoffrey’s
Cordial—an opiate mixture which in those times was often administered to
babies to keep them quiet.
It was, however, the notion of a link between economic crises, overpopulation, and excess mortality that took hold. Thus in 1898, in a study on commercial crises in England, Mijail Tugan-Baranovski concluded after a very superficial examination of the data that crises were associated with increased mortality. A much more careful study authored by William Ogburn and Dorothy
Thomas three decades later, in 1922, showed exactly the opposite, a positive
correlation of detrended annual series of business indicators and the mortality rate, which proved that economic depressions were associated with lower
mortality. Ogburn and Thomas were puzzled by this finding, but after much
Macroeconomic Effects on Mortality: Issues, Controversies, and Directions for Research
3
consideration and further study they thought it was real, as they found it
both in U.S. and British data.
MORTALITY AND THE BUSINESS CYCLE
The oscillations of economic activity between boom and bust, prosperity
and depression, or expansion and recession have been called business
cycles, trade cycles, industrial cycles, and crisis cycles, but such abundance
of terminology goes along with the inability of the economic profession
to agree on the causes of the phenomenon. In the 1860s, Clément Juglar
in Les Crises commerciales et leur retour periodique en France, en Angleterre,
et aux Etats-Unis and Karl Marx in Das Kapital theorized on the cause
of crises. Both attributed crises to the inner workings of the free-market
system, but their contributions had little resonance among economists who
were paying more attention to outstanding members of the profession
like W. S. Jevons and H. L. Moore, who attributed crises to influences of
the Sun or the planet Venus. It took a while for these astral theories to go
away, despite that they were clearly at odds with the facts. In 1920, an
economist-geographer, Ellsworth Huntington, proposed that recessions are
due to unidentified biological factors that generate peaks in mortality and
impact on the spending and investing psychology of the public. Huntington
was noticing the same correlation between death rates and macroeconomic
conditions that Ogburn and Thomas would notice later, but he was looking for causality in the opposite direction, that is, from mortality to the
economy.
In the 1930s, the world sank in depression and joblessness increased rapidly.
In Cycles and crisis, published in 1936, the German economist Wilhelm Roepke
wrote that the general contraction of economic activity of the depression was
associated with dismissed workmen, closed workshops, rusting machines,
and the human tragedies bound up with them, including a rise in death
rates. But, alas, he was totally wrong about this, as actually mortality had
decreased, puzzling public health workers (Tapia Granados & Diez Roux,
2009). It had been in the expansionary twenties that mortality had stagnated
or increased (Figure 1). However, at the time all this was barely registered.
After the depression and the war passed, new data now available made
obvious that mortality was secularly declining in many countries. In 1958, a
leading demographer and economist, George Stolnitz, claimed that disease
control, that is, advances in medicine and health care, had been the most
influential factor for mortality reduction. This was the typical view in the
1950s and 1960s, though the long-term decline in mortality was also thought
to be influenced by economic growth. Interestingly, in the United States, the
1950s and 1960s were economically prosperous but mortality declined at
4
EMERGING TRENDS IN THE SOCIAL AND BEHAVIORAL SCIENCES
22
20
18
16
14
12
10
8
6
Nonwhite
White
1920
1930
1940
1950
1960
1970
Figure 1 Age-adjusted mortality (per 100,000 population) for whites and
nonwhites in the U.S. civilian population, 1920–1970. Source: Historical Statistics
of the United States.
a much lower rate than in the 1930s and 1940s (Figure 1). The short-term
negative association between economic growth and mortality that Ogburn
and Thomas had discovered in the 1920s had been totally forgotten.
It was rediscovered in 1977 by a biologist at the University of Pennsylvania, Joe Eyer. By inspecting U.S. graphs of mortality and unemployment for
1870–1975, Eyer noticed that they evolved mirroring each other, so that peaks
in one series coincided with troughs in the other.
Eyer knew the 1920s publications by Dorothy Thomas and proposed several hypotheses to explain what he called the Thomas effect, that is, the rise
of mortality during economic expansions. He attributed it to higher levels of
stress at work, increasing overtime, overwork, and migration, and the subsequent decline in networks of social support and increase in the consumption
of harmful substances.
It was also during the 1970s that Thomas McKeown, a British historian
of medicine, published a series of analyses of population data. McKeown’s
basic conclusion was that population growth since the late eighteenth
century was mostly due to a drop in death rates caused by rising standards
of living. The basic mechanism would be a higher level of resistance to
infection due to an improvement in nutrition. For McKeown, better hygiene,
public health measures, and improved medicine had had only a limited
role in the historical decline of mortality. Though McKeown’s contributions
referred to long-term processes, and to the already gone time when most
deaths were due to infectious disease, they probably created a fertile ground
for the ideas of Harvey Brenner.
Brenner’s basic claim was that recessions raise mortality rates, though
the effect occurs, he said, with a lag. Brenner was very unclear about this
lag, stating in some papers it is just a few years, in others that it is 10
years, or even more. Given that recessions recur at variable periods—few
years or sometimes even more than a decade—this lagged effect cannot
Macroeconomic Effects on Mortality: Issues, Controversies, and Directions for Research
5
explain that troughs of mortality coincide with recessions, that is, with
peaks of unemployment. Brenner used econometric methods very obscurely
explained, and probably many readers, including reviewers, did not understand them. There were, however, researchers, starting with Eyer, who did
not buy Brenner’s main idea, that is, his “demonstration” of recessions
raising mortality with a lag. Brenner’s work was criticized as confusing and
irreproducible, but Brenner never answered his critics. All this was later
summarized as leading to considerable skepticism about Brenner’s data and
conclusions (Kasl & Jones, 2000).
PROCYCLICAL MORTALITY AS A CONTENTIOUS HYPOTHESIS
Since 2000, when Ruhm’s paper appeared, researchers from various fields of
social science have found in different countries and periods that over and
above long-term trends, mortality oscillates procyclically, that is, increasing
during expansions and decreasing during recessions—more than 30 of these
publications are cited elsewhere (Tapia Granados & Ionides, 2017). However,
incredulity persists among researchers who are reluctant to believe that recessions with the associated joblessness and loss of income are not harmful for
health and survival.
One of these investigators, Ralph Catalano, tested in a 1998 study the effect
of macroeconomic changes on mortality. As a kind of control, Catalano
included Danish data as a covariate in his models for the United States, an
unconventional method that no one has tried later. Catalano concluded that
mortality declined in years following increases in per capita national income
above long-term trend, that is, that expansions reduce mortality with a lag.
This is Brenner’s thesis with other words. However, Catalano seems to have
changed his views, as in recent controversies on the mortality effects of
the Great Depression (Bruckner, Noymer, & Catalano, 2013) and the Great
Recession (Tapia Granados & Ionides, 2016) he defended the view that
neither of them had any significant positive or negative effect on mortality.
In passing, it has to be said that maintaining that recession has no effect on
mortality while expansion stimulates its decline would not be admissible on
logical grounds.
In another controversy on the Great Depression, David Stuckler, Sanjai
Basu, and others argued that the only mortality effect of it was, as that
of other recessions, to raise suicides and reduce traffic fatalities, without
any detectable effect on major causes of death (Tapia Granados, 2013a).
These researchers reached this conclusion from investigating 1970–2007
data from 26 EU countries. This was a study that unfortunately conflated
data from two very different scenarios: the sustained decline of mortality rates—which indeed accelerated slightly during recessions—during
6
EMERGING TRENDS IN THE SOCIAL AND BEHAVIORAL SCIENCES
the 1980s and 1990s in Western Europe, and the demographic disaster
in Eastern Europe during the 1990s, when major increases in mortality occurred during the crisis transition to a market economy. Because
of the heterogeneity of the data, the study conclusions are hopelessly
unreliable.
It were also Stuckler and Basu, who in a book melodramatically entitled The
Body Economic—Why Austerity Kills, argued that during economic crises government policies determine whether mortality will increase or decline. Such
an optimistic view on the ability of government policy to modify quickly a
demographic variable as complex as mortality was a flawed diagnosis (Tapia
Granados, 2013b). It was demonstrated so by the fact that since 2008 mortality has significantly declined in Europe, particularly in Greece and Spain
where both the severity of the recession and the application of austerity policies have been outstanding (Regidor et al., 2016; Tapia Granados & Ionides,
2017; Tapia Granados & Rodriguez, 2015).
Further controversies on similar issues have occurred (Tapia Granados,
2014), and everything suggests that they will continue, as the sources of these
debates are well-rooted ideas. Doubtlessly, different investigators would
give different answers to the question of what specific misunderstandings
or erroneous ideas underlie these arguments. From the point of view of the
present writer, who is an interested party, two deep-rooted beliefs are the
basis of the visceral rejection of the hypothesis of procyclical mortality by
quite a number of investigators: first is the belief that a growing market
economy is good for everyone, something that economists have preached
since Adam Smith; second is the view that the level of income is the major
determinant of the probability of death, something that can be erroneously
inferred from modern public health research, which rather has shown that
working and living conditions and the social context—including what
epidemiologists call “social support,” —are key determinants of the risk of
death.
Looking at more superficial reasons for discrepancies, it is obvious that
sometimes they refer to misunderstandings on the analysis of time series
(Tapia Granados & Ionides, 2016), the nature of the business cycle, or the relation between causal structures and regression analysis. Thus in an investigation testing whether economic fluctuations have an impact on mortality, such
variables as traffic volume and tobacco consumption were included in a multivariate regression with the death rate as dependent variable (Economou,
Nikolaou, & Theodossiou, 2008). Since expansions can be harmful precisely
because they involve increased traffic and tobacco consumption, this is a perfect recipe for obtaining spurious results.
Complicating research on these issues and fueling skepticism is the fact that
methods to ascertain causal links between time-series variables have often
Macroeconomic Effects on Mortality: Issues, Controversies, and Directions for Research
7
raised controversy in social sciences, particularly in macroeconomics, where
major disagreements exist.
In early investigations of macroeconomic effects on health, the unit of
analysis was usually a whole nation, with the analysis reduced to a bivariate
analysis of time-series data. But most time series of economic indicators
and health variables are annual, and this usually means series that rarely go
beyond a hundred observations, and usually much shorter. Panel analyses
with disaggregated data for smaller geographical units have greater statistical power, but they raise two issues: what is the proper level of aggregation
(Lindo, 2015) and the violation of the assumptions of linear regression which
is caused by the use of linear trends and can bias the results (Ionides, Wang,
& Tapia Granados, 2013).
In 2015, Ruhm analyzed U.S. national-, state-, and county-level data
1976–2013 to investigate whether economic crises affect mortality “in the
same way as less severe downturns.” He concluded that the answer is yes,
so that both recessions and crises reduce death rates, with crises having an
effect on mortality that is about twice as strong as what would be expected
due to the elevated unemployment rates alone. In the operational definition
of economic crisis of this study, a crisis is just a severe recession as indexed
by unemployment reaching more or less arbitrarily determined “high
levels.” Ruhm admitted that this definition is arguable. For Wesley Mitchell,
the pioneer in business-cycle research, in the context of market economies,
“crisis,” “depression,” and “recession” are terms that refer basically to the
same phenomenon; they only suggest different intensities of it. On the other
hand, the famines that occurred in the USSR in 1932–1933, or in the Netherlands or India during World War II, or the extreme economic disruption that
occurred in Eastern Europe in the 1990s are also “economic crises,” in all
of which there were substantial increases in mortality. However, these are
economic crises of a very different nature to the recessions or depressions
of, say, the early 1980s or the last years of the past decade, which appeared
under “normal” social life in settled market economies. In all these cases,
mortality continued its secular decline, and dropped even faster.
A new example of the proneness of quite a number of researchers to
look for reasons to deny the procyclical oscillation of mortality is a recent
paper by Arthi et al. (2017) who propose a “migration bias” as the cause of
the “observed” procyclical oscillation of mortality. This oscillation would
actually be a statistical artifact. According to Arthi et al. (2017) selective
migration—toward booming regions and away from depressed areas—bias
the denominator of mortality rates causing mortality to seemingly oscillate
procyclically, when in reality it does not oscillates, or even oscillates countercyclically. The reasoning of the paper is tortuous, and its results are at
odds with many studies showing a procyclical oscillation of mortality using
8
EMERGING TRENDS IN THE SOCIAL AND BEHAVIORAL SCIENCES
national data (for instance in the USA, UK, Sweden, and Japan). But for sure
it will find a receptive audience.
POLICY ISSUES
Leading economists like Paul Samuelson, Milton Friedman, or Robert
Lucas claimed at different times the ability of economic policy guided by
macroeconomic principles to prevent major oscillations of economic activity.
However, the interventionist or laissez faire policies these authors advocated
were remarkably different. Indeed, the major economic downturns observed
around the turn of the century in most of the developing world and in
2008 in the global economy suggest that governments are rather unable to
prevent them. Furthermore, economists are seriously divided on what is to
be done to prevent or ameliorate recessions.
In spite of all that, some health researchers are convinced that it is government policy that determines whether an economic crisis will have or not
harmful effects on mortality. The idea is far from being demonstrated; indeed,
as has been argued here, the weight of evidence favors the view that mortality
oscillates procyclically, so that recessions stimulate the decline of mortality
independently of government policy.
Ruhm, who is arguably the contemporary researcher who has contributed
more to the view that expansions have harmful effects on mortality, has
claimed that contractionary macroeconomic policies are not justified, as
recessions “have overwhelmingly negative consequences, even if they
do not harm physical health.” Obviously, the negative consequences
meant by Ruhm are the business failures and the destruction of jobs
that characterize recessions and trigger social distress. But what about
policies intended to prevent the harmful effects of expansion? Ruhm
has suggested establishing economic incentives to reduce unhealthy
behaviors, and to promote healthier conditions of work—with reductions in overtime and mandatory expansion of vacation time. Policies
to reduce unhealthy consumption have been indeed implemented in
some countries, though almost exclusively for alcohol and tobacco products. Interestingly, in the field of public health, similar policies applied
to the consumption of fossil fuel have been recommended not only to
prevent climate change but also as potentially having major effects in
reducing traffic mortality, cardiovascular and respiratory diseases, and
many other causes of death. However, as illustrated by recent political
developments on climate change, in the short run the implementation
of such policies is very unlikely in any country, as they encroach on
business profits and therefore are strongly opposed by the business
community.
Macroeconomic Effects on Mortality: Issues, Controversies, and Directions for Research
9
Given disagreements inside economics on the effect of policies, the not
uncommon skepticism on the procyclical oscillation of mortality among
health researchers, as well as the scarce political feasibility of specific
policies to dampen the oscillation of mortality during expansions, to reach
any consensus to recommend this kind of policies seems very unlikely in the
near future. Thus, trying to develop theoretical foundations for such policies
does not look at all a fertile ground for work.
FIVE QUESTIONS THAT FUTURE RESEARCH SHOULD AIM
TO ANSWER
The starting point here is considering the procyclical oscillation of mortality
as a hypothesis supported by substantial evidence. For researchers who are
skeptical about it, what follows will probably make little sense.
1. What is the Connection Between the Epidemics of Prescription Drug
Poisoning, Other Iatrogenic Deaths, and the Business Cycle?
In the United States, the highly publicized epidemic of fatalities caused by
poisoning with prescription drugs seems to have grown with the recession,
that is, countercyclically (Ruhm, 2015). This epidemic of deaths caused
by prescribed medicines has obviously links with the larger chapter of
medical errors, estimated as the third leading cause of death in the United
States (Makary & Daniel, 2016). Now, all this raises the issue whether
business-cycle-related changes in the level of access or intensity of medical
care might be connected with procyclical mortality. According to reports of
the Centers for Disease Control (CDC), the overall U.S. death rate increased
in 2015 for the first time in a decade, exactly at the same time that Obamacare
was expanding access to health services. This is of course only one data
point, but it raises major questions.
2. Is Mortality Becoming Less Procyclical?
The procyclical oscillation of mortality might be disappearing because
dampening by the increasing weight in mortality of fatalities which are
either countercyclical (e.g., analgesic overdoses) or acyclical (cancer). Versus
this view, recent studies rather suggest the opposite. Lindo, in a study with
U.S. county data which provides important methodological insights has
found an intense procyclical oscillation of mortality and has rejected the
view that mortality would be becoming less procyclical (Lindo, 2015). Furthermore, in a number of studies, increased unemployment rates in recent
times (e.g., in U.S. states or EU nations) have been found associated with
10
EMERGING TRENDS IN THE SOCIAL AND BEHAVIORAL SCIENCES
large drops in mortality, which reinforce the hypothesis of procyclicality
of the death rate. At any rate, studies formally testing the hypotheses of
procyclical mortality and its potential dampening in recent times would
contribute to improve our understanding of these issues. China and India
are two countries in which testing these hypothesis would be particularly
valuable.
3. What are the Major Mechanisms for Procyclical Mortality?
Advances in understanding the mechanisms for procyclical mortality have
occurred. From an analysis of U.S. data, it has been concluded that about
a third of procyclical mortality is attributable to variations in atmospheric
pollution (Heutel & Ruhm, 2013). On the other hand, evidence that procyclical mortality due to injuries is connected with the procyclical oscillation of
industrial and recreational traffic as well as workplace activity and hiring
has continued piling up (Asfaw, Pana-Cryan, & Rosa, 2011; French & Gumus,
2014). Proposed connections between procyclical mortality and changes in
staffing of institutions for the elderly were suggested, but have been seen
with skepticism. A study using European data showed shorter working
hours associated with higher mortality (Johansson, 2004), a result that seems
to contradict the old idea that lower mortality in recessions may be linked to
the procyclical character of working time, overtime, and work-related stress.
However, this was just an isolated study, and indeed institutional factors
may modify the business-cycle character of hours worked, which may
measure different things in different countries. At any rate, the potential
relation of work hours, overtime, stress levels in the working environment,
and connected issues with the oscillation of mortality seems a largely
unexplored field worthy of investigation.
A still unpublished study has investigated the association of economic conditions in the area of residence with the level of risk factors for cardiovascular
disease in a sample of residents, finding that systolic and diastolic blood
pressure rise and physical activity drops during expansions. These can be
important findings opening major avenues for future research.
4. Who is Hurt, Who Benefits from Procyclical Mortality?
A recent study demonstrated that mortality decline significantly accelerated
in Spain during the recession that started in 2008 (Regidor et al., 2016). Mortality was found to be the highest in the group of low socioeconomic status
(SES) and the lowest in the group of high SES. The annual reduction in mortality during the recession years 2008–2011 was almost without exception
in each SES group greater than the reduction in 2004–2007, that is, during
Macroeconomic Effects on Mortality: Issues, Controversies, and Directions for Research
11
the previous expansion. Furthermore, the acceleration of mortality decline
during the recession was intense in the group of low SES, but very small in
the group of high SES. The conclusion was that mortality decline accelerated
during the recession, particularly in the group of low SES and, likely as a consequence of drops in the exposure to risk factors, probably more important
for individuals of low SES.
It seems that groups of lower SES benefit the most from the acceleration
of mortality decline during recessions. In the United States during the early
1930s, mortality dropped in whites and nonwhites and males and females,
but it dropped the most in African-American men (Tapia Granados & Diez
Roux, 2009). The mortality gap between whites and nonwhites had clearly
widened in the “roaring” 1920s, then narrowed in the depressed 1930s
(Figure 1). In Finland, in the severe recession of the early 1990s, mortality
declined the most among households obtaining income from manual
occupations (Tapia Granados, 2007). In Japan, stagnation during the 1990s
was associated with dramatic changes in occupational patterns of mortality,
as the health of managers and professionals deteriorated while that of sales
staff and blue collar workers did not, all of which led to a major reduction
or even reversal of the usual patterns of health inequality (Wada et al.,
2012). In all these studies, low SES groups benefit more from the reduction
in mortality during recessions, so that health inequality tend to diminish.
If that is the case, not only mortality but mortality inequalities would be
procyclical. A study with U.S. data (Edwards, 2008) seems at present the
only investigation perhaps inconsistent with the hypothesis that mortality
inequalities by SES are procyclical.
5. Is Economic Growth Presently Hindering Health Progress?
This is probably the most important question connected with the hypothesis
of procyclical mortality. It is a key question because economic growth as a
panacea for all social ills is an entrenched idea in our culture. So much so that
that two authors, Suchit Arora and R. F. Swift, “demonstrated” in the past the
cointegration between the level of health, as measured by life expectancy at
birth (LEB), and the level of income, as measured by GDP per capita. This
cointegration was also one of the “contributions” of Harvey Brenner.
Cointegration between LEB and income per capita means that in the long
run each variable will follow the path of the other, so that higher levels of
health will be obtained by raising levels of income. Versus that idea, supposedly proved by tortuous econometrics by Arora and Swift, what recent studies on the long-term evolution of mortality have shown is that, if there was
a positive link between economic growth and population health, that link
has disappeared in recent decades (Cutler, Deaton, & Lleras-Muney, 2006;
12
EMERGING TRENDS IN THE SOCIAL AND BEHAVIORAL SCIENCES
Preston, 2007). This is an idea that still provokes the suspicion and rejection
of those who more or less enthusiastically defend the thesis of “wealthier is
healthier” (Mackenbach, 2007).
The hypothesis of procyclical mortality is also counterintuitive because it
suggests that economic growth is harmful for health, while economic stagnation or contraction is beneficial. Thus an epidemiologist mocked once the
hypothesis of procyclical mortality by asking whether public health people
should advocate recessions. But, should they?
Let start from assuming that we agree that mortality is procyclical, so that
it deviates from a long-term declining trend upward in the expansions and
downward in the recessions. Now, this oscillation can be considered as having no net effect on the long-term evolution of mortality, as the excess mortality during the expansion may be compensated by lower mortality during
the recession. Then, in the long run, wider or flatter macroeconomic oscillations would make no difference in the evolution of mortality. But in most
business cycles, the expansion is longer than the recession, and therefore the
above-trend mortality of the expansion would not be compensated by the
below-trend mortality during the recession. If that is the case, longer or faster
expansions would mean a longer accumulation of over-trend mortality; that
is, faster or more maintained GDP growth would cause slowly increasing or
even decreasing LEB, while longer or deeper recessions would mean longer
accumulation of below-trend mortality, that is, faster increase of LEB. Quite
substantial evidence seems to support this hypothesis.
With one of the oldest and best demographic statistics of the world,
Sweden has been the object of many demographic studies and controversies.
Using Swedish data, Edward Ionides and I showed in 2008 that in the past
two centuries there was a reversal of the relation between economic growth
and health progress. Throughout the nineteenth century GDP growth was
positively associated with the annual decline in mortality, or the gain in
LEB, but the relation became weaker as time passed and was completely
reversed in the second half of the twentieth century, when economic growth
appears inversely associated with health progress, with higher annual GDP
growth implying lower annual reductions in mortality, or gains in LEB.
This paper, like those by Arora and Swift, have been basically unnoticed
by health researchers. Unfortunately, published research is often ignored
rather than replicated or refuted, which does not contribute to scientific
progress.
While the hypothesis that economic growth has become a hinder for health
progress is clearly supported by the case of Sweden, additional “circumstantial evidence” is abundant from other countries and periods. Thus in
the UK, Amartya Sen showed an inverse relation between the decennial
rate of GDP growth in the period 1900–1960 and the decennial increase of
Macroeconomic Effects on Mortality: Issues, Controversies, and Directions for Research
13
LEB in England and Wales (Sen, 2001), a finding that was later replicated
for a larger timeframe of almost two centuries. In the United States, the
decades prior to the Civil War of the 1860s saw rapid economic growth at the
same time that the stature of native-born white males dropped, revealing
a deterioration of population health (Haines, Craig, & Weiss, 2003). Then,
in the twentieth century, during the “roaring” 1920s, mortality stagnated or
increased, while in the depressed 1930s it quickly dropped, and during the
“prosperous” 1950s and 1960s it basically stagnated (Figure 1). In the two
most populous nations of the world, China and India, the past half century
saw quick mortality decline in the decades of economic stagnation and slow
mortality decline when economic growth accelerated (Cutler et al., 2006).
The relation seems to be observed also in African countries, where high GDP
growth has been associated with poor improvements in infant mortality and
other health indicators in recent decades. Thus Botswana and South Africa
had much higher GDP growth and much smaller reductions in mortality
than Morocco and Ethiopia.
According to World Bank data, in 2014 Japan was the nation with the
highest LEB (83.6 years), followed by Spain, with the highest LEB in Europe
(83.1 years). Now, the remarkable thing is that these two countries have had
a very poor economic performance in recent decades, with Japan basically in
chronic stagnation since the 1990s and Spain suffering the worst recessions
and the highest levels of unemployment in Europe since the early 1980s. The
recent Great Recession has been associated with major gains in LEB in Spain,
Greece, and the Baltic States, that is, the economies where the recession was
the most severe. Contrarily, among the high-income countries of the OECD,
the United States and Denmark have been often considered as perhaps
the most efficient economies in term of flexible and well-performing labor
markets which allow more sustained GDP growth and less unemployment.
At the same time, though, both countries are the OECD laggards in terms of
population health.
The common view that business prosperity and GDP growth are what we
need to solve social problems seems at odds with the aforementioned facts,
but it is also questioned by something more important, the fact that faster
GDP growth means both at the level of national economies and the global
economy, greater emissions of CO2 (Tapia Granados, Ionides, & Carpintero,
2012) and thus a faster approximation toward what could be the worst
human-made catastrophe in history. Of course, advocates of zero growth
usually ignore the obvious fact that in our economic system no growth
represents rising unemployment rates and social malaise. But those who are
enthusiastic about economic growth are very often oblivious to the harmful
consequences of it.
14
EMERGING TRENDS IN THE SOCIAL AND BEHAVIORAL SCIENCES
The function of social science, Joan Robinson once said, “is quite different
from that of the natural sciences—it is to provide society with an organ of
self-consciousness.” Let us hope that humanity may generate a sufficient
level of self-consciousness before it goes down into a man-made black hole.
Perhaps research on the macroeconomic effects on health can contribute
something to that endeavor.
REFERENCES
Arthi, V., Beach, B., & Hanlon, W. (2017). Estimating the recession-mortality relationship when migration matters. NBER Working Paper 23507.
Asfaw, A., Pana-Cryan, R., & Rosa, R. (2011). The business cycle and the incidence of
workplace injuries: Evidence from the U.S.A. Journal of Safety Research, 42(1), 1–8.
Bruckner, T. A., Noymer, A., & Catalano, R. A. (2013). Life expectancy during
the Great Depression in eleven European countries. Population and Development
Review, 39(1), 57–74.
Cutler, D., Deaton, A. S., & Lleras-Muney, A. (2006). The determinants of mortality.
Journal of Economic Perspectives, 20, 97–120.
Economou, A., Nikolaou, A., & Theodossiou, I. (2008). Are recessions harmful to
health after all?: Evidence from the European Union. Journal of Economic Studies,
35(5), 368–384.
Edwards, R. D. (2008). Who is hurt by procyclical mortality? Social Science & Medicine,
67(12), 2051–2058.
French, M. T., & Gumus, G. (2014). Macroeconomic fluctuations and motorcycle fatalities in the U.S. Social Science & Medicine, 104, 187–193.
Haines, M. R., Craig, L. A., & Weiss, T. (2003). The short and the dead: Nutrition,
mortality, and the "antebellum puzzle" in the United States. Journal of Economic
History, 63(2), 382–413.
Heutel, G., & Ruhm, C.J. (2013). Air pollution and procyclical mortality. NBER Working
Paper. 2013(18958).
Ionides, E., Wang, Z., & Tapia Granados, J. A. (2013). Macroeconomic effects on mortality revealed by panel analysis with nonlinear trends. Annals of Applied Statistics,
7(3), 1362–1385.
Johansson, E. (2004). A note on the impact of hours worked on mortality in the OECD.
European Journal of Health Economics, 4, 335–340.
Kasl, S. V., & Jones, B. A. (2000). The impact of job loss and retirement on health. In L.
F. Berkman & I. Kawachi (Eds.), Social epidemiology (pp. 118–136). New York, NY:
Oxford University Press.
Lindo, J. M. (2015). Aggregation and the estimated effects of economic conditions on
health. Journal of Health Economics, 40, 83–96.
Mackenbach, J. P. (2007). Did Preston underestimate the effect of economic development on mortality? International Journal of Epidemiology, 36(3), 496, 497; 502–503.
Makary, M. A., & Daniel, M. (2016). Medical error—the third leading cause of death
in the US. BMJ, 353.
Macroeconomic Effects on Mortality: Issues, Controversies, and Directions for Research
15
Preston, S. H. (2007). On ’The changing relation between mortality and level of economic development’. International Journal of Epidemiology, 36(3), 502–503.
Regidor, E., Vallejo, F., Tapia Granados, J. A., Viciana-Fernández, F. J., de la Fuente, L.,
& Barrio, G. (2016). Faster mortality decline in low socioeconomic groups during
the economic crisis: Authors’s reply. Lancet, 389, 1794–1795.
Ruhm, C.J. (2015). Health effects of economic crises. NBER Working Paper 21604.
Sen, A. (2001). Economic progress and health. In D. Leon & G. Walt (Eds.), Poverty,
inequality, and health: An international perspective (pp. 333–345). Oxford, England:
Oxford University Press.
Tapia Granados, J. A. (2007). Case Study A2: Do health inequalities increase when
employment grows? In J. Benach, C. Muntaner & V. Santana (Eds.), Employment
conditions and health inequalities - Final report to the WHO Commission on Social Determinants of Health (CSDH) prepared by the Employment Conditions Knowledge Network
(EMCONET). Geneve, Switzerland: WHO.
Tapia Granados, J. A. (2013a). Health and the Great Depression: A reply to Stuckler
et al. Journal of Epidemiology and Community Health, 67(12), 1073–1074.
Tapia Granados, J. A. (2013b). A flawed diagnosis: Book review of The Body Economic:
Why Austerity Kills. Science, 341, 1176–1177.
Tapia Granados, J. A. (2014). The Great Recession, a cause of health improvement?
Salud Colectiva (Buenos Aires), 10(1), 101–108.
Tapia Granados, J. A., & Diez Roux, A. V. (2009). Life and death during the Great
Depression. Proceedings of the National Academy of Sciences of the United States of
America, 106, 17290–17295.
Tapia Granados, J. A., & Ionides, E. L. (2016). Statistical evidence shows that mortality
tends to fall during recessions: A rebuttal to Catalano and Bruckner. International
Journal of Epidemiology, 45(5), 1683–1685.
Tapia Granados, J. A., & Ionides, E. L. (2017). Population health and the economy:
Mortality and the Great Recession in Europe. Health Economics.
Tapia Granados, J. A., Ionides, E. L., & Carpintero, O. (2012). Climate change and
the world economy: Short-run determinants of atmospheric CO2 . Environmental
Science & Policy, 21, 50–62.
Tapia Granados, J. A., & Rodriguez, J. M. (2015). Health, economic crisis, and austerity: A comparison of Greece, Finland and Iceland. Health Policy, 119(7), 941–953.
Wada, K., Kondo, N., Gilmour, S., Ichida, Y., Fujino, Y., Satoh, T., & Shibuya, K. (2012).
Trends in cause specific mortality across occupations in Japanese men of working
age during period of economic stagnation, 1980–2005. BMJ, 344, e1191.
JOSÉ TAPIA GRANADOS SHORT BIOGRAPHY
José A. Tapia Granados joined Drexel University after spending 11 years
as a Researcher and Lecturer at the University of Michigan in Ann Arbor.
Prior to that, he lived and worked in New York City, Baltimore, Washington, D.C., and Madrid, Spain, where he practiced medicine briefly as a primary care doctor. Working at the World Health Organization headquarters
16
EMERGING TRENDS IN THE SOCIAL AND BEHAVIORAL SCIENCES
in Washington, D.C. brought him to the United States in 1989. His research
and teaching focus on the intersection of public health, economic issues, and
social science.
RELATED ESSAYS
The Great Recession and Young Adults’ Labor Market Outcomes around the
World (Sociology),Arnaldo Mont’Alvao and Monica K. Johnson
Inefficiencies in Health Care Provision (Economics), James F. Burgess et al.
Labor Market Instability, Labor Market Entry, and Early Career Development (Sociology), Michael Gebel
The Reorganization of Work (Sociology), Charles Heckscher
Family Formation in Times of Labor Market Insecurities (Sociology), Johannes
Huinink
Social Network Analysis in the Study of Ethnic Inequalities (Psychology),
Frank Kalter
Social, Psychological, and Physiological Reactions to Stress (Psychology),
Bruce S. McEwen and Craig A. McEwen
Health and Social Inequality (Sociology), Bernice A. Pescosolido
Limits to Human Longevity (Sociology), Samuel H. Preston and Hiram
Beltrán-Sánchez
Social Relationships and Health in Older Adulthood (Psychology), Theodore
F. Robles and Josephine A. Menkin
The Role of Cultural, Social, and Psychological Factors in Disease and Illness
(Sociology), Robert A. Scott
Incarceration and Health (Sociology), Christopher Wildeman